



Personnel safety considerations
There are several routes of exposure to HDs. HDs can enter the body via inhalation, accidental injection, ingestion of contaminated foodstuffs, hand-to-oral contact, and dermal absorption.30 While HD exposure is always a constant threat when chemotherapeutic agents are used, proper procedures and policies can minimize the risk. The United States Pharmacopeia (USP) has developed an enforceable “General Chapter” practice standard devoted to the handling of HDs, which outlines standards regarding personnel protection for preparation and handling of HDs. Because an indepth discussion of HD controls is beyond the scope of these guidelines, readers can refer to USP for more detailed information on this topic.
Veterinary practices will ordinarily not be involved in chemotherapeutic drug compounding. However, it is helpful for the healthcare team personnel to have a general awareness that direct contact with HDs, either by handling, reconstituting, or administering HDs, represents an exposure risk.31 Many HDs have also been found to have drug residue on the outside of drug containers, which creates another opportunity for exposure of individuals who receive drugs and perform inventory control procedures.32 Personal protective equipment (PPE) should be used to protect personnel from exposure during handling of HDs. PPE includes gloves, gowns, goggles for eye protection, full face shield for head protection, and respiratory barrier protection.
Regular exam gloves are not recommended for use as standard protocol for handling chemotherapeutic agents. However, as an expedient, wearing two pairs of powder-free nitrile or latex gloves can be used as a last resort. Vinyl gloves do not provide protection against chemotherapy. Ideally, gloves should be powder free and rated for chemotherapy use by the American Society for Testing and Materials (ASTM). For receiving HDs, one pair of ASTMtested chemotherapy gloves may be worn.31 When administering, managing, and disposing of HDs, two pairs of ASTM-tested chemotherapy gloves may be worn.31 The inner glove should be worn under the gown cuff and the outer glove over the cuff. Disposable gowns made of polyethylene-coated polypropylene or other laminate materials offer the best protection.31
Eye, face, and respiratory protection is mandatory when working with HDs outside of a clean room or isolator cabinet, or whenever there is a probability of splashing or uncontrolled aerosolization of HDs. A full face mask is a suitable alternative to goggles, although it does not form a seal or fully protect the eyes. A NIOSH N95 respirator mask is suitable for most situations, with the exception of large spills that cannot be contained by a commercially available spill kit.
PPE should be removed in the following order: chemotherapy gown (touching the outside of the gown, then rolling the outside inward to contain HD trace contamination), goggles and face shields (touching only the outside without making contact with the face), then chemotherapy gloves (touching the outside of the gloves away from the exposed skin while attempting to roll the glove outside-in). If a glove becomes contaminated or if there is a breach in the glove, it should be removed and discarded promptly, while carefully avoiding contamination of the handler’s skin or nearby surfaces.
Closed system transfer devices (CSTDs) are another type of PPE that can be used for any cytotoxic chemotherapy agent (although not necessarily for all HDs) during preparation and administration. In the case of non-cytotoxic agents that are not on the NIOSH list of HDs, for example, asparaginasej, a CSTD is not required. FDA approval of CSTDs requires the following capabilities: no escape of HDs or vapor, no transfer of environmental contaminants, and the ability to block microbial ingress. CSTDs can greatly reduce the potential for HD exposure to clinical personnel and should always be used concurrently with other PPE.
Traditional needle and syringe techniques for mixing HDs create the potential for droplet or aerosol contamination with the drugs that are being handled. CSTDs prevent mechanical transfer of external contaminants and prevent harmful aerosols that are created from HDs mixing from escaping and exposing personnel.30 CSTDs are commercially available from a number of companies k,l,m,n.
The following additional safety precautions will help minimize the potential for exposure of personnel handling HDs:
- Male and female employees who are immune-compromised or attempting to conceive, and women who are pregnant or breast feeding, should avoid working with chemotherapy agents.
- Employees or pet owners who will be exposed to the patient’s waste (urine, feces, vomit, blood) within 72 hr of chemotherapy administration (sometimes longer for some drugs) should wear proper PPE.
- Chemotherapy pills (tablets and capsules) are best handled within a biological safety cabinet (BSC) if available. If no BSC is available, a ventilated area or a respirator should be used to avoid inhalation of HD particles or aerosols.
- Separate pill counters should be used for chemotherapy pills. Counters labeled for chemotherapy use will help avoid inadvertent use with conventional medications. The counters should be stored either within the BSC (not to be removed) or in a sealed container (i.e., a plastic box with secure lid) dedicated to that pill counter and any other items that may come in contact with HD pills.
Environmental safety considerations
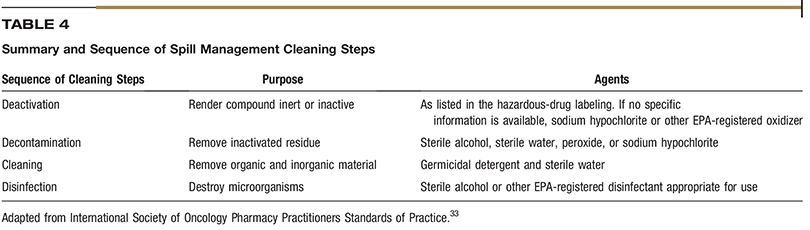
Environmental controls are an important part of risk mitigation. The recommended location for chemotherapy preparation and administration is a quiet, low-traffic room that is dedicated to chemotherapy purposes, free from distractions, and easy to clean. Because HD spill events represent the greatest risk of personnel exposure, it is important to use extreme care when cleaning spills. Commercially available spill kits are useful in containing and cleaning HD spills. Absorbent pads or pillows can be used to immediately contain larger spills. When managing a spill, it is recommended to start from the outer edges of the spill and work your way towards the middle to prevent spreading HD residue. A HD-spill management sequence (Table 4) has been developed and is a suitable basis for a veterinary practice protocol.33 Spill kits should contain instructions for use and be located in areas where HDs are located and administered. Only trained personnel should cleanup HD spills and should be wearing appropriate PPE, including double chemotherapy gloves and respiratory masks.
HD agents are best stored in a dedicated, closeable cabinet or refrigerator. Following administration, discard HDs, administration materials, and gloves and other PPE into chemotherapy waste receptacles. It is important that staff members who have touched chemotherapy vials or potentially contaminated areas NOT touch anything or anyone else until they have removed their PPE and washed their hands.
Labeling of hazardous drugs
Labeling of HDs is an extremely important aspect of personnel safety. Without adequate HD labeling, personnel are placed at risk of accidental exposure to HDs. All HDs should be labeled clearly with chemotherapy warning labels. Injectable HD agents should be labeled as “opened” or “reconstituted” on a specific date and the concentration of the reconstituted agent should be indicated.
“Look-alike, sound-alike” describes drugs that are spelled and pronounced similarly but are different. The term came about in response to errors involving inadvertent misfills of drugs, for example, vincristine being confused with vinblastine. A simple practice that many pharmacies now follow is arranging their medication stock alphabetically by generic name using a “Tall Man Lettering System.”37 This is a simple way to emphasize spelling and pronunciation differences between drugs (e.g., vincristine is written as vinCRIStine and vinblastine is written as vinBLAStine.)37
Appropriate labeling of mixed chemotherapies can also reduce errors and allow for another double check prior to administration. Diluted drugs should be labeled with the amount of drug in milligrams contained in the syringe or minibag. For drugs that are not diluted, it is good practice to label the syringe with the concentration of the drug as it comes from the vial. These labeling techniques allow for another double check prior to administration.
The Institute for Safe Medical Practices has developed several strategies to prevent simple errors. Naked decimal points and trailing zeros have been implicated in many errors in healthcare and have been designated as unapproved abbreviations.38 An example of a naked decimal point is when “0.2 mg” is written as “.2 mg,” easily leading to a 10-fold overdose if “.2 mg” is read as “2 mg.” Similarly, a trailing zero notation is when “10 mg” is written as “10.0 mg,” which can easily be mistaken for “100 mg.”