Beyond pain management: Treating the cause of canine OA

Canine osteoarthritis (OA) is one of the most common chronic conditions affecting dogs of all ages. Traditionally, its management has centered on providing pain relief, which is understandable given the clear impact on a dog’s mobility and quality of life. However, a growing body of research and experience suggests that this pain-centric approach may be too narrow.
Sponsored content by Exubrion Therapeutics
It’s time to reframe arthritis not just as a painful condition, but as a disease of rampant inflammation. In recognizing the inflammatory nature of OA and adopting a proactive treatment strategy that is aimed at modulating the inflammatory process, veterinarians can provide more effective, long-term care.1-3
Advertisement
Understanding the nature of canine osteoarthritis
Inflammation in osteoarthritis affects the entire joint—cartilage, synovium, subchondral bone, and surrounding tissues—and plays a central role in the disease’s progression. Cytokines, prostaglandins, and matrix metalloproteinases (MMPs) are released in response to joint damage, which then perpetuate a vicious cycle of inflammation that causes pain and structural degradation.1,2
Importantly, this inflammatory cascade begins well before pain becomes evident, and dogs may have significant joint pathology before showing any outward signs. In fact, studies have shown that radiographically visible OA is very common in young dogs. In one study, radiographic OA was found to be highly prevalent in dogs aged 8 to 48 months, with 60% of these dogs clinically affected.4 Clearly, waiting for clinical signs of pain often delays meaningful intervention.
Recognizing the limitations of a pain-centric approach
Relying solely on pain as the guide for treatment is problematic as it is subjective, often under-recognized by owners, and is not always an accurate reflection of the underlying joint pathology that is slowly degrading the joint.
Unfortunately, the traditional approach to canine OA has largely focused on strategies to treat pain, such as NSAIDs, gabapentin, and anti-nerve growth factor (anti-NGF) injections. While these modalities offer some benefits, they aren’t designed to treat the underlying cause of the disease. At best, they may buy time and potentially improve quality of life. At worst, they provide insufficient relief or carry risks that limit long-term use.5
This raises a critical question: What if we could directly target the inflammation driving the disease? By shifting the clinical focus from reactive pain management to a proactive “inflammation-forward” approach, veterinarians can better hope to preserve joint function and improve long-term outcomes.
Adopting a proactive, inflammation-forward strategy
Identifying at-risk dogs early is the first step in effective OA management. This includes large breeds, working dogs, those with joint injuries, or those genetically predisposed to hip or elbow dysplasia. Diagnostic tools such as radiography, gait analysis, and owner questionnaires (eg, LOAD or COAST scores) can help detect early disease, even before pain becomes obvious. Early intervention, particularly when the signs are subtle, offers the best chance of controlling inflammation before irreversible damage occurs.
Educating owners is also key. For an inflammation-forward approach to succeed, pet parents need to be actively educated to seek help before the pain has become pronounced enough to limit their dog’s quality of life. Helping to reframe this perception requires owners to understand that:
- Arthritis is not just painful—it’s a progressive, inflammatory disease
- The earlier we intervene, the better the outcome
- We need to go beyond pain relief and specifically address the inflammation that is causing it in the first place
Going deeper to treat the source of OA pain and debilitation
Synovetin OA®, a colloid containing microparticles of the radioisotope tin-117m, is an intra-articular veterinary device now available at practices across the US. It represents a paradigm shift: from managing symptoms by masking pain to breaking the vicious cycle of inflammation and helping to reduce pain at the source, while also preserving the health of the joint.1,3,6,7
Synovetin OA is injected directly into the affected joint. Once there, it delivers targeted radiotherapy to activated macrophages in the synovium and synovial fluid—the very cells that perpetuate inflammation in OA.1,3,6,7
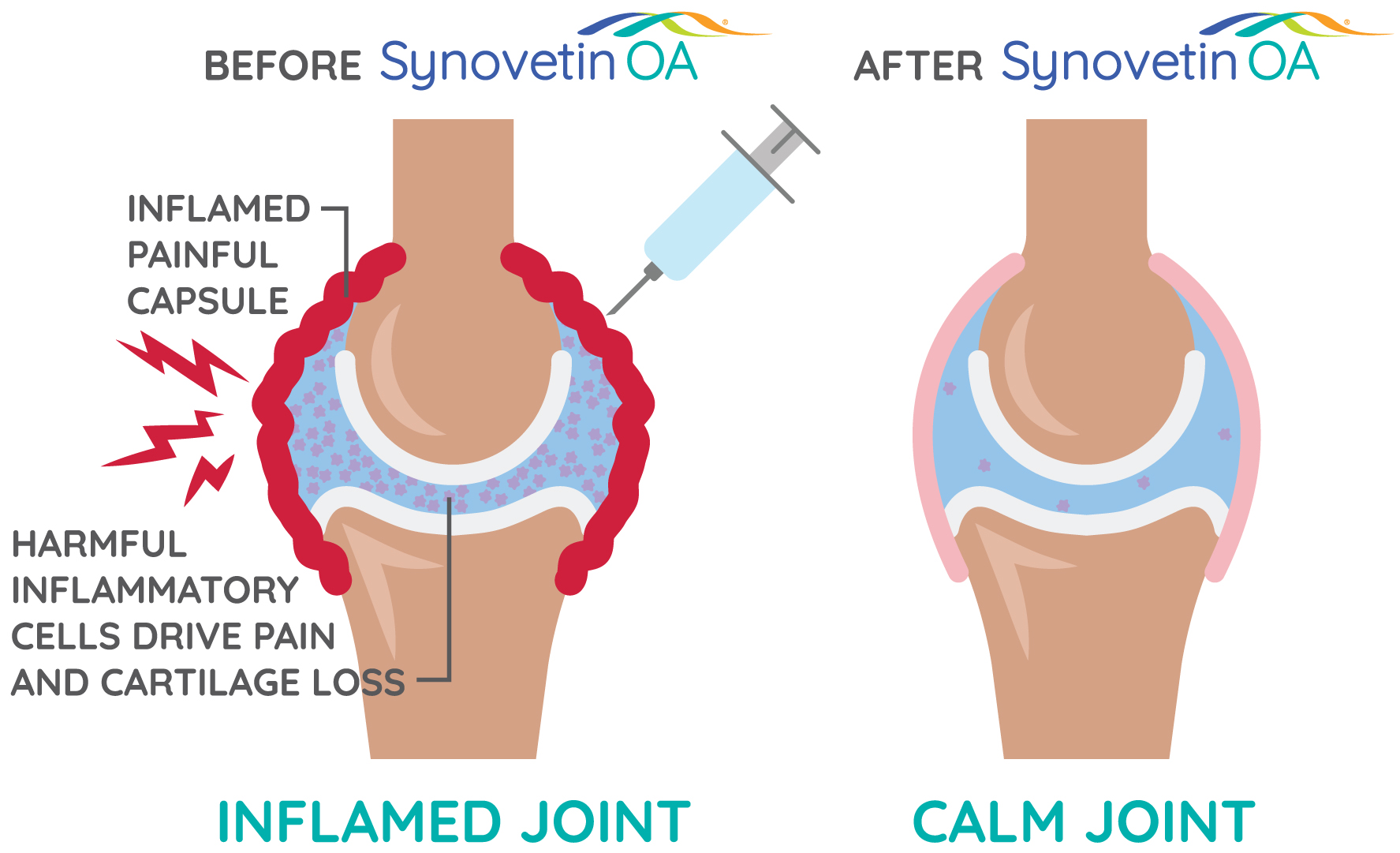
Tin-117m conversion electrons are low energy, with a short tissue penetration range which is ideal for treating synovitis without affecting cartilage, bone, and other joint structures. Following treatment, inflamed, painful synovial cells (synoviocytes) take up the microparticles. The emitted energy from tin-117m deactivates these cells, helping to restore the synovium and providing pain relief. Macrophages in the synovial fluid also engulf the microparticles and are subsequently eliminated. This reduces the production of cartilage damaging cytokines, thus breaking the destructive cycle at its source.1,6-8
This approach to OA management offers advantages to veterinarians and pet parents alike: 1,3,6,7
- One simple, minimally invasive, outpatient treatment provides up to one full year of relief
- Exceptionally safe with no systemic side effects for treated dogs
- No pet parent compliance issues that come with daily medications or monthly veterinary visits
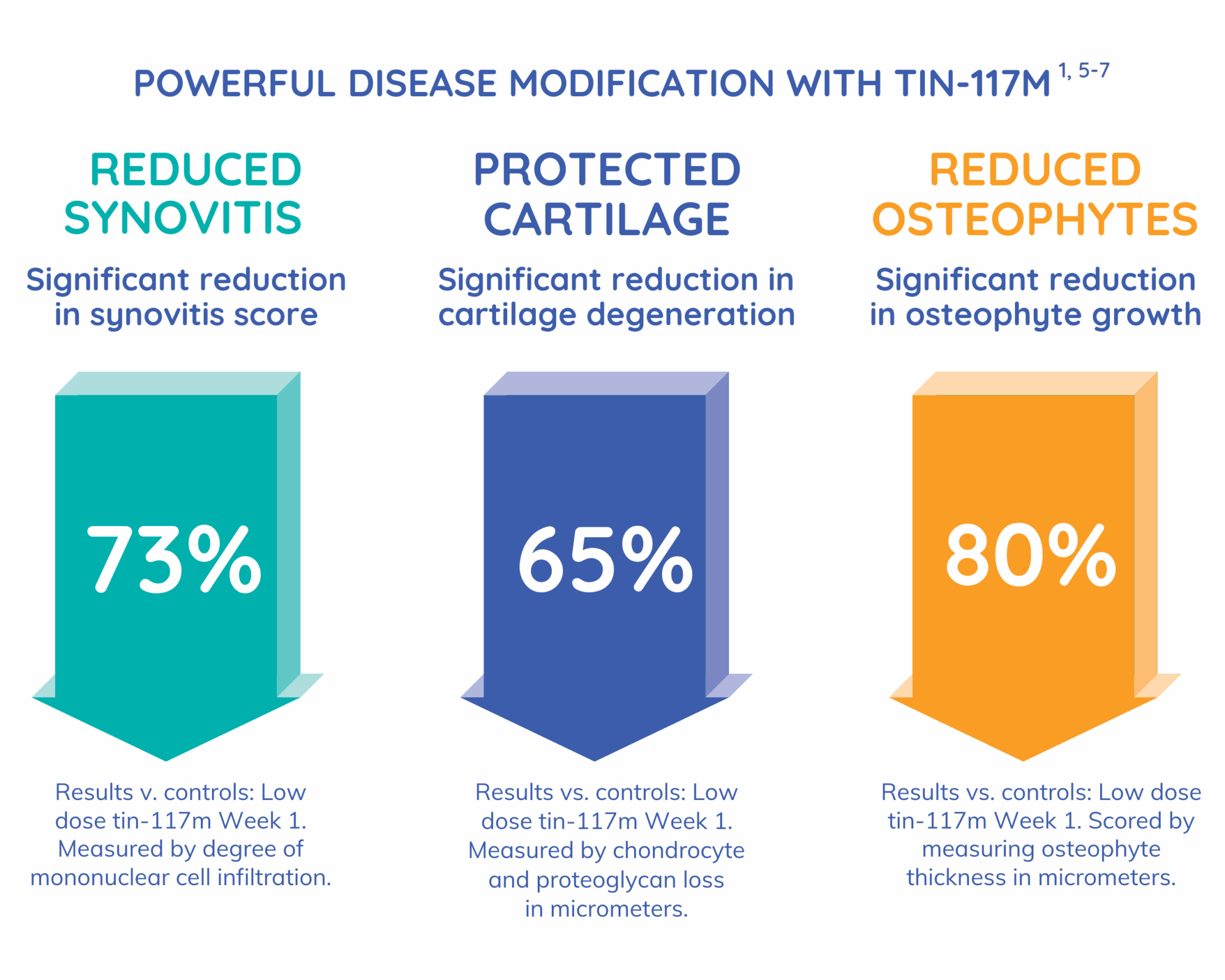
Newly published research demonstrates the powerful disease-modifying effect of tin-117m
Preclinical studies in rodent models have shown evidence that tin-117m has the potential to slow disease progression, with substantial reductions in synovitis, cartilage erosion, and bony remodeling observed. This raises the question: “Is Synovetin OA a disease-modifying osteoarthritis treatment?” Time will tell, but these findings are promising—and exciting.1
Summary: Shifting the mindset, changing the outcomes
For veterinarians and pet parents alike, Synovetin OA offers new hope with an inflammation-forward approach. “This innovative therapy allows us to address osteoarthritis not just as a source of pain, but as an inflammation-driven degenerative disease (synovitis)—one that can potentially be modified or slowed at any stage,” says Matthew Brunke, DVM, DACVSMR (Canine), CCAT, Sports Medicine and Rehab Specialist, Veterinary Referral Associates, an AAHA practice. “I’ve seen the results myself after treating approximately 200 dogs with Synovetin OA. This could be especially beneficial in early OA where the targeted action provides an opportunity to relieve pain and break the vicious cycle that leads to disease progression.”
While pain relief remains a critical goal, it should be seen as a downstream outcome of controlling the inflammatory process. By shifting the focus from pain relief to inflammation control, veterinarians have the opportunity not only to relieve suffering but to extend the active, happy years of their canine patients.
Learn more:
To find out how Synovetin OA can fit into your OA treatment strategy, visit Synovetin OA® or contact Eric Schreiber, Chief Commercial Officer, at [email protected].
LOAD, Liverpool Osteoarthritis in Dogs; COAST, Canine OsteoArthritis Staging Tool.
References:
1. Bendele A, Doerr CA, Gonzales GR, et al. Front. Vet. Sci. 2025;12:1-13 doi: 10.3389/fvets.2025.1621296. 2. Sokolove J, Lepus CM. Ther Adv Musculoskel Dis. 2013;5(2):77-94. 3. Aulakh KS, Lopez MJ, Hudson C, et al. Vet Med (Auckl). 2021. Jun 4;12:117-128. doi: 10.2147/VMRR.S295309. PMID: 34113552; PMCID: PMC8187093. 4. Johnson SA. Vet Clin North Am Small Anim Pract.1997;27(4):699-723. 5. Farrell M, Waibel FWA, Carrera I, et al. Front Vet Sci. 2025;12:1581490. 6. Donecker J, Fabiani M, Gaschen L, Aulakh KS. PLoS One. 2021. Jul 19;16(7):e0254613. doi: 10.1371/journal.pone.0254613. PMID: 34280212; PMCID: PMC8289027. 7. Donecker J, Lattimer JC, Gaschen L, Aulakh KS. Vet Med (Auckl). 2021. Dec 17;12:325-335. doi: 10.2147/VMRR.S345144. PMID: 34950571; PMCID: PMC8691448. 8. Stevenson NR, Lattimer J, Selting K, et al. Abstract S6-03. World J Nucl Med. 2015;14(Suppl 1):S15-S68.
