Clinical
Risky business? Using a risk-based approach to stay safe amid HPAI H5N1

From driving to the clinic in the morning to taking radiographs, every moment of our lives and practice involves some element of risk. Without even thinking about it, we are constantly assessing risk and doing what we think is necessary to mitigate risk. We put on our seatbelts, stop at red lights, use lead protective gear when taking radiographs, and chemically immobilize a fractious patient to keep them and veterinary staff safe.
Advertisement
To figure out your strategy to mitigate the risk posed from a patient with HPAI H5N1 (the hazard), let’s think through the risk. Risk is a function of likelihood and consequence. How likely is it for that hazard to take place—exposure to HPAI? If you are exposed, how severe is the consequence? According to the Centers for Disease Prevention and Control (CDC), the human health risk is low for the general public; however, risk increases with exposure to infected animals or contaminated environments.
Today, our focus is on H5N1, but tomorrow it could be a completely different threat. By adopting a risk-based approach to how we assess and respond to situations, we will be better prepared – not just for H5N1, but for any emerging zoonotic disease.
Likelihood of Exposure
According to the CDC, while “human infections with HPAI (H5N1) virus are rare, unprotected exposure to infected animals or contaminated increases the risk of infection.” To date, minimal infections have been reported among humans—most, according to CDC, associated with unprotected exposures to infected animals, including poultry and dairy cattle.
In a 2024 study assessing the risk of a HPAI H5N1 isolate using a ferret model, Restori et al found that the primary modes of transmission were direct contact (75% of exposed ferrets) and airborne transmission (37.5% of exposed ferrets), with evidence of disease transmission at a low infectious dose, and virulence at low doses. So, what does this mean in practice? It doesn’t take a large dose of the virus to become infected. That’s why it is important to think about how we reduce the likelihood of exposure– by addressing contact risk (minimizing contact with infected animals and contaminated environments), and by taking steps to lower the risk of airborne transmission.
Consequences of Exposure
According to the CDC, illnesses in people from HPAI A (H5N1) range from mild (upper respiratory, conjunctivitis) to severe (pneumonia, organ failure, death).
In practice, we are also concerned about the risk of exposure to other patients.
An additional concern is that the spread of H5N1 opens up new opportunities for the virus to undergo mutations and reassortment during replication that could potentially increase its transmissibility, pathogenicity, and virulence. To date, there have been no confirmed cases of human-to-human transmission in the current outbreak. However, ongoing infection prevention and control measures are essential to mitigate the risk of mutations or reassortments that could enable such transmission.
Systematic Approach to Risk Mitigation
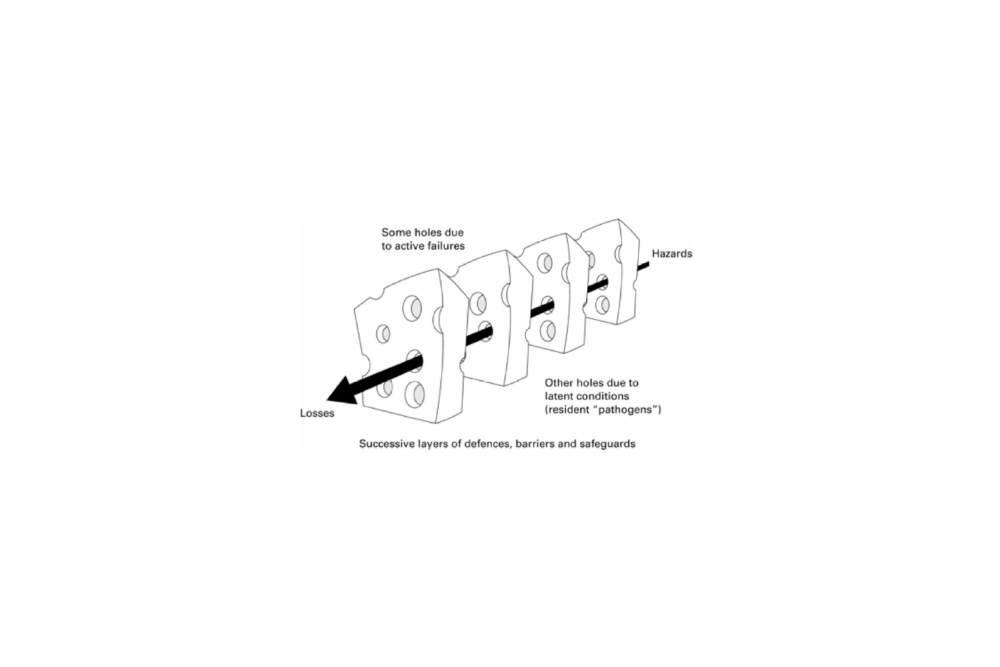
Reducing risk requires a layered approach. Aside from being able to completely guarantee that no H5N1 patients will show up to your hospital (which is probably impossible), there is no way to eliminate risk. Instead, we use a range of strategies to reduce both the likelihood and consequence of exposure.
Like Reason’s Swiss Cheese Model shown here, the idea is that by blocking enough different holes (multiple approaches to risk mitigation), the overall risk is reduced. For example, an N95 mask without fit-testing may not fully protect against exposure if it’s not properly fitted. Likewise, purchasing disinfectants that are effective against H5N1 is not enough if staff aren’t trained on their proper use or if a disinfection protocol isn’t in place. Any one of these interventions on their own may be insufficient, but the sum of these practices will greatly reduce overall risk.
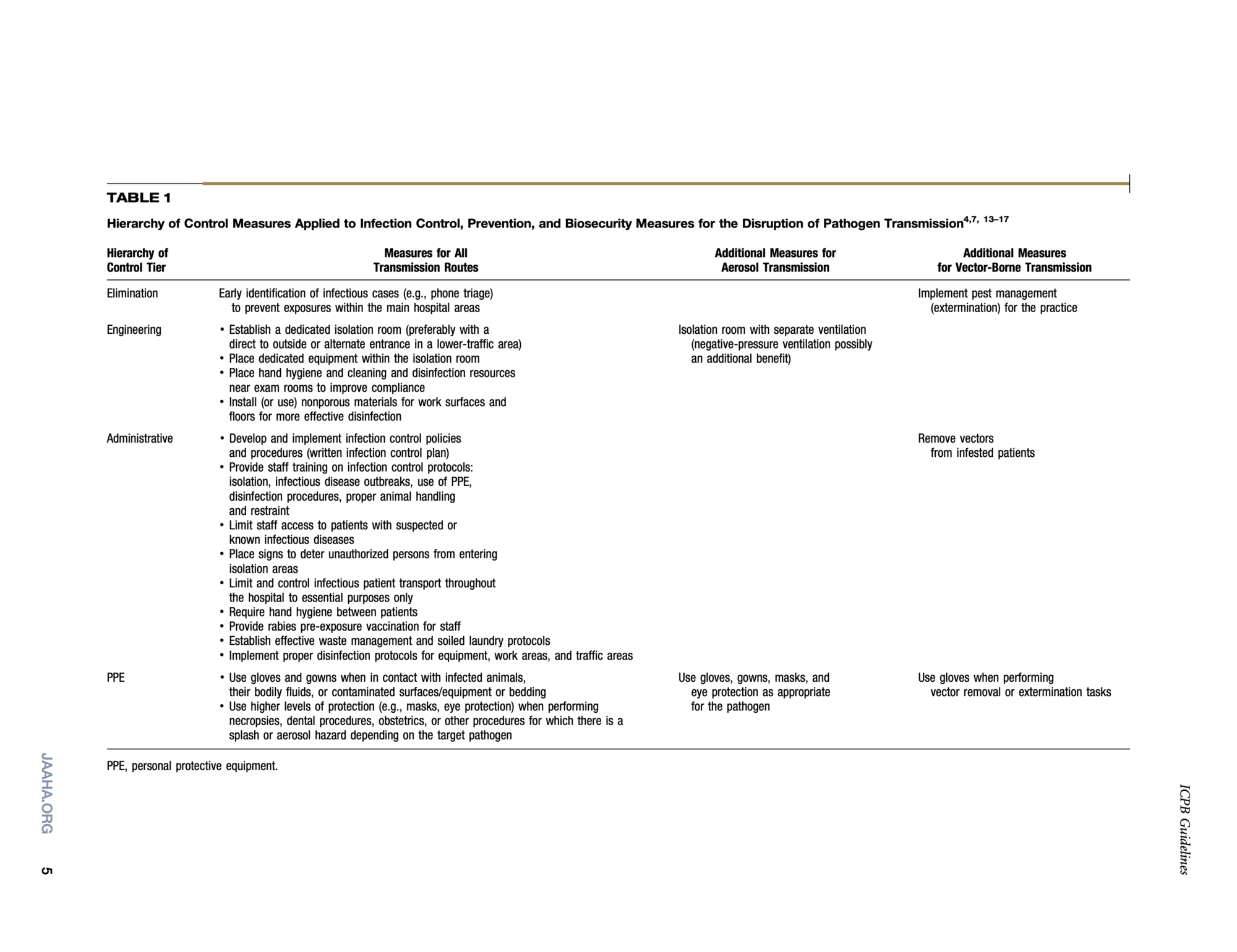
When controlling risk, we use a hierarchy of controls approach—ranking strategies from most to least effective. The most effective approaches involve hazard elimination or substitution, followed by engineering controls, administrative controls, and at the bottom of the hierarchy, personal protective equipment (PPE).
The following chart from our 2018 AAHA Infection Control, Prevention, and Biosecurity Guidelines shows how to apply this approach in a veterinary clinic setting in a way that can be applied across different types of pathogens. CDC has links to different strategies specific to H5N1; many items are farm related.
The Minnesota Department of Health has developed infection prevention and control guidance for veterinarians and veterinary staff who may be in close contact with companion animals suspected or confirmed to have H5N1. The guidance offers practical recommendations for clinics, including screening questions during appointment scheduling to identify potential cases, strategies for isolating affected animals, and protocols for using PPE and dedicated equipment to reduce transmission risk to both staff and other patients.
Specifics for PPE
It may be surprising to see PPE as a less effective strategy compared to other types of controls. Effective PPE requires a combination of standard operating procedure (SOP; administrative controls) and the appropriate PPE. What is nice about PPE is it really comes down to a practical, common-sense approach that can be easily taught to staff: if there is a contact risk—wear gloves, gowns, and shoe covers; if a patient has respiratory signs, think about how to protect your mucous membranes (goggles, mask). Of course, the specific types of gloves and masks matter—we all remember those cloth masks used during the early days of COVID-19. Cloth masks never really caught on as a fashion trend, and more importantly, though they may have helped reduce some droplet spread, they didn’t offer sufficient protection against most droplet and airborne transmission.
Here is the CDC’s list of recommended PPE you need if working around H5N1. The CDC emphasizes the need for extra precautions during dentistry and procedures that may cause aerosolization of the virus:
- Disposable or non-disposable fluid-resistant coveralls or gown*, and depending on task(s), add disposable or non-disposable waterproof apron
- Any NIOSH Approved® particulate respirator (e.g., N95® or greater filtering facepiece respirator, elastomeric half mask respirator with a minimum of N95 filters)
- Properly-fitted unvented or indirectly vented safety goggles** or a face shield if there is risk of liquid splashing onto the respirator
- Rubber boots or rubber boot covers with sealed seams that can be sanitized or disposable boot covers for tasks taking a short amount of time
- Disposable or non-disposable head cover or hair cover
- Disposable or non-disposable gloves
* Preferably, fluid-resistant coveralls should be made of material that passes:
- AATCC 42 ≤ 1 g and AATCC 127 ≥ 50 cm H2O or EN 20811 ≥ 50 cm H2O; or
- ASTM F1670 (13.8 kPa); or
- ISO 16603 ≥ 3.5 kPa
** Preferably, safety goggles should conform to ANSI Z87.1 that are marked at least Z87 D3
Making Risk Reduction Fun: Handwashing and PPE Donning/Doffing Activities for Your Team
We need more than just PPE stored in a box in our supply closet—it is important to ensure staff know how to properly put it on and take it off to prevent contamination. The following table, from AAHA’s 2018 guidelines, serves as a helpful reminder for you and your staff on the correct procedures for putting on and removing PPE safely.
One fun way to practice this with your team is to apply shaving cream to their gloves (or full gown/gloves/shoe covers) and have them practice donning and doffing—see where else that shaving cream shows up at the end and how safe they were. Public Health Ontario has a fantastic activity guide to practice handwashing and PPE use. Glo Germ and your woods lamp/UV light can also be great for checking handwashing technique.
Consider setting up a time each month to run one of these activities. These exercises will not only help your staff stay safe when treating H5N1 cases but also help strengthen your overall infectious disease prevention and control capabilities and reduce the risk of unintentional pathogen exposure to your staff and patients.

Fit-testing: What is it and how do we get this done?
The CDC and public health agencies recommend a “well fitted NIOSH approved” respirator and emphasize that fit-testing of respirators is important. There are different ways to conduct fit-testing to make sure that the respirator (i.e. N95) is sealed and does not allow for exposure.
While human medical facilities routinely conduct fit-testing, it is not as widely adopted in veterinary practice. It is very important to recognize, in terms of both safety and liability. The Occupational Safety and Health Administration (OSHA) (29 CFR 1910.134) “requires respirator users to be fit tested to confirm the fit of any respirator that forms a tight seal on your face before using it in the workplace.” Fit testing is required annually or when there are changes that may impact how well a mask fits (i.e. weight change, a cosmetic surgery, etc). In fit-testing, you may learn that some staff need different brands of masks to ensure a proper seal. Companies can be contracted to come perform fit-testing at your practice. Local VMAs, your state public health veterinarian or others may be able to help your clinic find out where and how to get your staff properly fit-tested. OSHA has a comprehensive guide for small entities on developing a respiratory protection standard (fit testing described starting on page 35).
Disinfection
Disinfection, as we all know from cleaning up more cages that we can count, isn’t just about which chemicals work on what. As veterinarians, we may know better than any other profession that you need to clean off the dirt, feces, fur —whatever the cat dragged in—before you disinfect.
Michigan has a great handout on disinfecting for HPAI that includes both protocols and which agents to use. Agents include:
- A phenolic disinfectant (like Pine-Sol) solution
- Virkon-S or accelerated hydrogen peroxide (AHP), commonly known as Accel or Rescue
- Bleach (such as Clorox) at a rate of 1:32, which is 1/2 cup (4 oz.) to one gallon of water. Dish or laundry soap can be added to the mixture. Do NOT add ammonia to bleach/water mixture
Summary
When you are thinking of H5N1 (or any other hazard), if you can use the
risk=likelihood x consequence approach—you can quickly come up with some common-sense approaches. Consider:
- What is the likelihood of exposure?
- How can I minimize that likelihood with a swiss cheese model of administrative procedures (protocols, training), engineering controls (mechanical devices, air flow), PPE (types, use)?
- For reducing H5N1 exposure likelihood, we shared tools for improving admin controls associated with PPE through activities, fit-testing and links to CDC recommendations and AAHA guidance on infection control.
- What is the consequence?
- How can I reduce the consequence (or can I?)?
- Consequence reduction for H5N1
- We can reduce consequences in our patients who are ill through supportive care.
- We can vaccinate ourselves and recommend our staff keep up to date on seasonal flu vaccines to possibly reduce the risk of viral mixing (reassortment).
- We can monitor staff health and send exposed staff with signs/symptoms to get checked at their provider.
- Depending on location, the state/local health department may reach out to staff exposed to H5N1 to interview them about interactions with the patient and may be able to arrange for testing.
- If exposed staff seek health care through their providers if they develop symptoms, it will be important they share the possible exposure with their provider
Situational Update:
| Species impacted: | Cases: | Where: | How is it transmitted/spread?* | What to look for: |
|---|---|---|---|---|
| Domestic cats | 136 in U.S. since 2022 | 21 states: CA, CO, IA, ID, IL, IN, KS, LA, MI, MN, MO, NE, NJ, NM, OH, OK, OR, PA, SD, TX, UT, WA, WY | •Eating infected birds & rodents
•Eating raw meat or poultry products/ commercial pet food or unpasteurized milk •Contact with infected cattle/poultry and their contaminated environments •Contact with infected people or contaminated clothing and/or infected people possible but not established |
•Anorexia
•Lethargy •Fever •Oculonasal discharge •Difficulty breathing •Neurologic signs (ataxia, circling, tremors, seizures, blindness). •Can be rapidly fatal (up to 70% of infected cats die of their infections); however, serosurveys have reported antibodies to H5 viruses in ~12% of apparently healthy stray cats |
| Dogs (companion) | 0 in U.S. | Canada
Washington study detected H5 and N1 antibodies in 2% of hunting dogs |
•Eating infected birds | •Anorexia
•Fever •Conjunctivitis •Cough •Difficulty breathing |
| Poultry (includes backyard chickens and ducks) | Detected in 1,683 flocks; > 168 million birds affected in U.S. since 2022 | 50 states & Puerto Rico (commercial and backyard flocks and live bird markets) | •Contact with infected poultry or wild birds
•Contact with contaminated equipment •Contact with infected people or contaminated clothing •Poultry trade promotes spread |
•Acute mortality
•Respiratory signs (sneezing, coughing, oculonasal discharge) •Edema of the face and cyanosis of combs and wattles •Diarrhea •Skin hemorrhages •Decrease in egg production •Neurological signs (tremors, stargazing, paralyzed wings) |
| Cattle | 1,007 since 2024 | 17 states: AZ, CA, CO, ID, IO, KS, MI, MN, OH, OK, NV, NM, NC, SD, UT, TX, WY | •Contact with infected animals
•Contact with contaminated milking equipment and clothing (large amounts of virus shed in the milk) •Exposure to infected wild birds (Nevada and Arizona)** |
•Many subclinical or mild infections (unlike poultry) making detection difficult
•Thickened, abnormal milk •Loss of appetite •Lethargy •Low-grade fever •Mild respiratory signs •Diarrhea (less common) |
| Swine | 2 cases since first detection in 2024 | One state: OR | •Contact with infected animals
•When infected by cows, unlikely to infect other swine •Fomites/contaminated equipment |
•Coughing
•Fever •Respiratory signs •Loss of appetite •Lethargy •Abortions |
| Sheep | 0 in U.S. | Reported case in England | •Exposure to infected birds | •Mastitis, with no other clinical signs, was reported in this case |
| Wildlife | > 500 species globally (485 avian and 48 mammalian species)
U.S. wildlife cases are reported by the USDA and U.S. Geological Survey |
50 states, Puerto Rico | •Consumption of sick prey (mammals and birds)
•Direct transmission & contact with contaminated environments (including virus in water) for wild avian flocks •Rare reports of transmission between wild mammals |
Clinical signs in sick wildlife are variable, but generally include neurologic and respiratory signs.
Sick wild birds can have: •Eye swelling •Change in color of iris •Respiratory signs (sneezing, coughing, oculonasal discharge) •Gastrointestinal signs (diarrhea) •Neurologic signs (tremors/seizures) The most common clinical signs in sick wild mammals are: •Neurologic signs (tremors/seizures and ataxia) •Respiratory signs (nasal and ocular discharge and dyspnea) |
| People | 70 cases in the U.S. in the past year | 13 states: CA, CO, IO, LA, MI, MO, NV, OH, OR, TX, WA, WI, WY | •No sustained human-human transmission
•Contact with sick cattle & poultry •One North American fatality had genotype primarily found in wild birds •CDC study detected H5N1 antibodies in 2% (3/150) of bovine veterinary practitioners |
•Conjunctivitis
•Fever •Cough •Sore throat •Runny or stuffy nose •Muscle aches •Fatigue •Shortness of breath or difficulty breathing •GI signs (diarrhea, nausea, vomiting - less common) •Seizures (less common) |
The numbers represent reported cases, not the actual number of affected individuals.
* Information on modes of transmission are suspected or verified based on reported evidence for each species. In general, avian influenza viruses can be transmitted through direct contact, indirect contact (e.g., contaminated surfaces), and inhalation.
**The HPAI virus initially detected in dairy cattle, H5N1 clade 2.3.4.4b genotype B3.13, was the only strain known to infect dairy cattle. However, in early 2025, two spillover events involving a different genotype circulating in migratory birds, D1.1, occurred in dairy cattle in Nevada and Arizona. Ongoing new introductions will complicate efforts to control the virus in dairy cattle, underscoring the importance of robust surveillance and prevention measures.
RESOURCES:
AAHA
2018 AAHA Infection Control, Prevention, and Biosecurity Guidelines
Minnesota Department of Health
Influenza A(H5N1) Infection in Companion Animals – Guidance for Pet Owners
Colorado Department of Public Health & Environment, Communicable Disease Branch
California Department of Public Health
What Veterinarians Need to Know about Bird Flu
Testing and Management of Cats for Influenza: Guidance for Veterinarians
Veterinary Provider Letter Influenza A Testing in Cats
Centers for Disease Prevention and Control
Swiss Cheese Model
Reason J. 2000. Human error: models and management. BMJ. 2000;320:768–70. doi: 10.1136/bmj.320.7237.768.
Additional Resources and Further Reading
APHIS/USDA HPAI Detections in Mammals
APHIS/USDA Avian Influenza Detections in Po
APHIS/USDA Avian Influenza Detections in Wild Birds
AVMA News Study: Three bovine veterinarians unknowingly infected with H5N1
CDC Summary of Avian Influenza
CDC Information for Workers Exposed to H5N1 Bird Flu
Cornell University Highly Pathogenic Avian Influenza (Bird Flu) Resource Center
Restori, K.H., Septer, K.M., Field, C.J. et al. 2024. Risk assessment of a highly pathogenic H5N1 influenza virus from mink. Nat Commun 15, 4112. https://doi.org/10.1038/s41467-024-48475-y
USGS Avian Influenza in Wildlife
USGS Avian Influenza Surveillance in Wildlife
Photo credit: EyeEm Mobile GmbH via Getty Images / iStock
Disclaimer: Trends content is meant to inform, educate, and inspire by providing an array of diverse viewpoints. Any content published should not be viewed as an official stance, position, or endorsement by the American Animal Hospital Association (AAHA) or its Board of Directors.
