Vaccination Risk-Benefit Assessment
Risk assessment variables when determining an individualized vaccination plan from the 2020 AAHA/AAFP Feline Vaccination Guidelines.

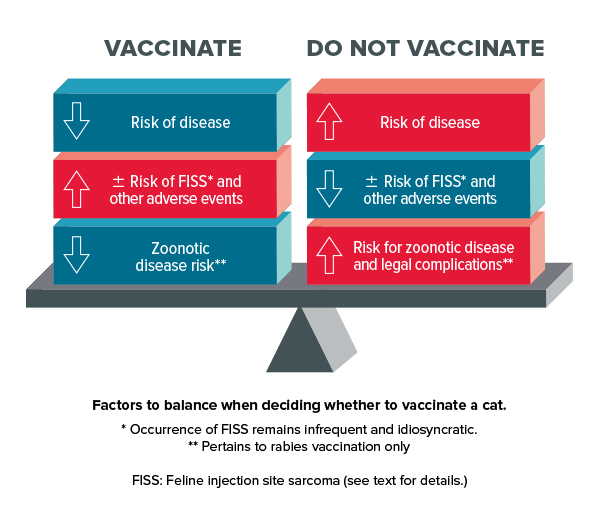
A Balancing Act
There is always a balance to be struck when considering risks associated with vaccination and benefits of vaccination for the individual patient:
- A decision to vaccinate might involve a young cat residing in a multi-cat household with outdoor access, living in an area with a known high prevalence of the pathogen being vaccinated against.
- A decision not to vaccinate might involve a senior or geriatric cat residing in a single-cat household with no outdoor access, and a vaccine that has poor efficacy against a pathogen with low virulence or limited local prevalence.
To download infograph, click here.
The Task Force supports the WSAVA’s recommendation that veterinarians should vaccinate every animal with core vaccines and give non-core vaccines no more frequently than is deemed necessary.2 The decision whether or not to administer a vaccine to a cat, and how frequently, relies on an individual case-by-case assessment by the veterinarian. This involves consideration of the animal, the animal’s environment, and the pathogen in question. Additionally, risk-benefit assessments should consider the safety of the vaccine, other adverse effects of vaccination (e.g., the effect of feline immunodeficiency virus vaccination on in-clinic diagnostic test kits), and the efficacy of the vaccine. The result of this assessment should be an individualized, evidence-guided recommendation to vaccinate or not to vaccinate.
TABLE 6
Risk Assessment Variables Determining an Individualized Vaccination Plan
For a printable PDF, click here.
| RISK FACTORS | Considerations |
|---|---|
| Age and life stage | Susceptibility, MDA, activity level, reproductive status |
| Health status | Concurrent disease, nutritional status, level of parasitism |
| Agent exposure | Geographic prevalence, cat lifestyle, housing |
| History | Adverse vaccine events, response to vaccination by littermates, previous desease |
| Immunodeficiency | Congenital or acquired (including chronic stress) |
Patient’s Characteristics
Age is an important factor in assessing an individual’s risk profile. In contrast to puppies, kittens born to immune queens appear to lack transplacentally acquired antibodies and instead absorb specific MDA through colostrum,4 which provides important protection during early life. Once MDA have waned, however, kittens become susceptible to infection. Most infectious diseases are more prevalent in kittens than adults, and therefore, kittens (in particular, those younger than 6 months old) represent a principal primary target population for vaccination. Conversely, adult cats generally have a more robust adaptive immune response when challenged (assuming they are healthy and not immunocompromised), whether due to previous natural exposure or vaccination, and age-related resistance to challenge is particularly a feature of FeLV infection.26 Consequently, vaccination of mature cats is generally considered less critical than vaccination of kittens. The presence of concurrent disease or stress causing immunosuppression should also be a consideration prior to vaccination because this may affect an animal’s susceptibility to infection and response to vaccination.
Patient’s Environment
Population density and opportunity for exposure to infectious agents are two critical issues that should form part of the risk-benefit assessment. In general, cats and kittens living in larger multi-cat households and environments (e.g., boarding, breeding, foster, or shelter facilities) have a higher risk of infection than cats living in oneor two-cat households. In addition to the possible presence of infected animals acting as reservoirs for infection in multi-cat households, the immunosuppressive effects of stress associated with high-density feline housing may result in reactivation of some infections as well as increased susceptibility to new infections. The introduction of new cats into multi-cat households also increases the risk of infectious disease not only to the cat entering the household but also to the whole group because of possible direct exposure to new infectious agents.
When assessing the opportunity for exposure to a given pathogen for an individual cat, the lifestyle of the cat and other cats in the same household needs to be considered. It is critical to determine whether the cat is indoor-only or has outdoor access (including supervised outdoor visits on a harness, or boarding) because cats with outdoor access may be at increased risk of pathogen exposure. Indoor-only cats, however, may still be determined to be at risk of exposure to pathogens, either from other cats in the household (i.e., subclinically infected or carrier cats), or by fomite transmission of pathogens brought in from outside on the owner’s body, clothing, or shoes. Indoor-only cats may also be exposed to infectious agents when brought to a veterinary clinic for a wellness examination. In theory, strictly indoor cats may be more susceptible to developing some infectious diseases (such as FPV and FCV infection) than cats with outdoor access because they may not receive “natural boosting of immunity” that occurs with natural exposure.1
The geographic distribution of infectious agents may also result in different risks of exposure (e.g., rabies), and therefore, questions regarding future travel should be included in determining the risk of exposure to specific infectious agents.
Infectious Agents
The likelihood of infection and disease is influenced by pathogen factors such as virulence, strain variation, and challenge dose (i.e., how many infectious units of exposure). The need for vaccination is greatest against pathogens with high virulence, such as FPV, and pathogens that cause widespread morbidity, such as FHV-1.
Boehringer Ingelheim Animal Health USA Inc., Elanco Animal Health, Merck Animal Health, and Zoetis Petcare supported the development of the 2020 AAHA/AAFP Feline Vaccination Guidelines and resources through an educational grant to AAHA.



