



Development of a Training Program for Law Enforcement K9 Handlers to Administer Naloxone

From the Jul/Aug 2020 issue. Subscribe today to get your copy
by Ashley Mitek, DVM, MS, DACVAA; Maureen McMichael, DVM, MEd, DACVECC*; Brad Weir, MD, FAAEM, FACEP, FAEMS; Michael Smith, MD, NRP, FAEMS, FAAEM; Danielle Schneider, BA; David Schaefer, MS, PhD
From the Department of Veterinary Clinical Medicine, University of Illinois College of Veterinary Medicine, Urbana, Illinois (A.M., M.M., D.S., D.S.); and Department of Emergency Medicine, Carle Illinois College of Medicine, Urbana, Illinois (B.W., M.S.).
Correspondence: [email protected] (A.M.)
Accepted for publication: December 11, 2019.
*M. McMichael’s present affiliation is the Department of Clinical Sciences, College of Veterinary Medicine, Auburn University, Auburn, Alabama.
IM (intramuscular); IN (intranasal); LEK9 (law enforcement K9); LEO (law enforcement officer)
ABSTRACT
As the opioid epidemic continues across the United States, law enforcement K9s (LEK9s) are at increased risk of accidental exposure and overdose. This study evaluated a novel training program teaching handlers to administer naloxone to their LEK9 in the event of an overdose. Seventy-five LEK9 handlers from a governmental agency attended a naloxone training session. A presurvey given to the handlers evaluated their knowledge of opioid overdose in LEK9s and their confidence administering naloxone. Officers were educated via a PowerPoint presentation about naloxone and how to administer it to their LEK9. A postsurvey evaluated changes in their knowledge and confidence as a result of the presentation. Sixty-two presurveys and 47 postsurveys were completed. Nearly all handlers had never given their LEK9 an intramuscular or intranasal injection. Most handlers were not comfortable monitoring their LEK9’s vital signs for an opioid overdose. After the training, handlers demonstrated a mild increase in comfort level administering intramuscular and intranasal naloxone (15 and 14% increase, respectively). Comfort level monitoring vital signs and symptoms of an opioid overdose increased 38 and 32%, respectively. Handlers may not be fully prepared to assess and treat their LEK9 and may benefit from a targeted training program teaching them to administer naloxone.
Disclaimer
- The information contained within is not intended to diagnose or treat a patient. It is provided for educational purposes only.It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. The authors are not responsible or liable for any advice, course of treatment, diagnosis, or service.
- There are only a select number of states that have legalized the treatment of animals by nonveterinarians. In many instances, the provision of medical services by a nonveterinarian may violate the Veterinary Practice Act of a state, or other legislation. We recommend the reader review their state’s laws before providing medical care to a law enforcement K9 (LEK9), and have the name and number for a contact veterinarian(s) in the area. For a comprehensive review of the legalities of first responders treating LEK9s, we direct readers to a thorough manuscript by Hanel et al.1 Real-time updates on changes in laws affecting the transport or treatment of LEK9s can be found at workingdogHQ.com.
- Injured, conscious LEK9s may pose a serious health risk to the personnel working around them; they can exert a bite force of 500–800 psi.2 The risk of injury to human personnel can be significantly reduced by the correct placement of a basket muzzle. No attempt at naloxone administration, transport, or first aid should be rendered to an LEK9 until a basket muzzle is in place.Unconscious LEK9s administered naloxone may wake up in an excitatory state, posing safety risks to unprepared personnel.
- The treatment of an overdosed LEK9 should not prevent a human from being treated with naloxone.
- When approaching the scene of a suspected opioid-overdosed LEK9, providers should wear personal protective equipment gloves to prevent contact with potent opioids. Mouth-to-snout ventilation should NOT be attempted in these situations to avoid human harm or death from residual substances in or around the nose and mouth.
Introduction
In October 2016, three narcotic detection law enforcement K9s (LEK9s) inhaled trace amounts of fentanyl powder in carpet fibers and overdosed in the line of duty. The LEK9s became drowsy and unresponsive to commands and were transported to a veterinary hospital, where they were resuscitated with naloxone.3 It is unknown exactly how many LEK9s experience opioid overdose in the field because there is no national database and no mandatory reporting. In an important work, Palmer and Gautier outlined the risk of synthetic opioid toxicity in LEK9s and discussed the use of naloxone as an antidote.4
To combat the opioid epidemic raging across the United States, LEK9s will continue to be at increased risk of overdose. This risk has increased significantly in past years as a direct result of the availability of more potent illegal opioids. Heroin, which had been the primary illegal opioid identified, is twice as potent as morphine.5 However, fentanyl is approximately 100 times more potent than morphine,6 and carfentanil, another opioid being added to street drugs, is 10,000 times more potent than morphine.5 Fentanyl and related synthetic opioids are appearing more frequently in drugs being sold as “heroin.”
Human opioid overdoses treated in the emergency room rose by 30% from 2016 to 2017.7 In particular, the Midwest saw a 70% increase in opioid overdoses during this time frame.7 In 2016, there were 42,249 accidental deaths due to opioid overdose, and opioids were responsible for 66% of all deaths due to drug overdose.8 This spike in death rate compared with previous years has been linked to illegally manufactured fentanyl, which experts believe is being added to heroin and cocaine street drugs, in addition to methamphetamines and other compounds.8 Owing to ease of manufacturing (e.g., made in a laboratory versus growing poppies in a field) and distribution (e.g., the more potent the product, the smaller the package), it is possible that the epidemic will get worse.
The opioid epidemic has prompted many municipalities to require their first responders to carry naloxone. Many law enforcement officers (LEOs) currently carry naloxone and are trained to administer it to a human. In one elegant study, Ray et al. demonstrated that LEOs had overwhelming positive feelings about being trained to use naloxone, and the officers reported they had little difficulty in administration.9 A study evaluating a naloxone training program for humans reported that training LEOs in naloxone administration can increase knowledge and confidence in managing opioid overdose emergencies. In addition, LEOs have shown that they can safely administer naloxone via intransal route.10,11
Naloxone can be administered in several ways. For a comprehensive review of the studies evaluating route of administration and dose of naloxone in LEK9s, we direct readers to the thorough Palmer and Gautier 2017 clinical update.4 Intranasal (IN) and transmucosal naloxone administration studies have not been published for canines, although research indicates these routes work well in humans. An unpublished study found that IN naloxone works well in canines (personal communication with C. M. Otto, Penn Vet Working Dog Center, School of Veterinary Medicine, University of Pennsylvania, Philadelphia, PA, 2018). For the purposes of this training, we focused on teaching handlers to administer naloxone intramuscular (IM) and IN, because these two routes require minimal training.
In 2016, a law enforcement agency raised concerns about potential exposure to their LEK9s after they reviewed documents from the Federal Bureau of Investigation and Department of Homeland security warning all LEK9 handlers in the United States to be aware of a possible opioid overdose in the line of duty.3 After initial consultation with the K9 unit, we developed a Naloxone Training Program to be administered at the annual in-service LEK9 handler training. Because there would be a significant time delay from the time the agency requested educational material for their handlers to when we could provide the face-to-face training, we created an online video demonstrating how to identify and treat an opioid overdose in an LEK9 (creative commons, free to use and distribute here.12 This video has more than 10,000 views and is currently being used to train LEK9 handlers and first responders across the nation and is recommended by the CDC for training any K9 handler.
Given the increased risk of opioid overdose, the cost of one LEK9 (typically upwards of $10,000), and the emotional bond between handler and K9, veterinarians should ensure that all handlers are equipped and educated to provide the antidote to their LEK9 in an emergency situation in accordance with the laws of their jurisdiction.
The goals of this study were to establish current knowledge levels of handlers relating to the administration of naloxone to an LEK9 via a pretraining survey, to provide focused training on IM and IN naloxone administration, and to evaluate changes in handler comfort level and knowledge after training with a short postlecture survey.
Our hypothesis was that a brief training session on opioid overdose in LEK9s, including recognition of symptoms and appropriate treatment, would improve the handlers’ knowledge and comfort in treating an exposed LEK9.
Materials and Methods
Prior to the training session, we created the Working Dog Task Force, which included veterinarians, physicians, and K9 handlers. Expertise from these three respective fields enabled the development of practical training materials. A 25 min PowerPoint lecture was created that covered the relative potencies of opioids circulating on the street, the symptoms of opioid overdose in LEK9s, the importance of human safety when approaching a suspected K9 overdose victim, and the recommended treatment, including various routes of administration. A PDF of the presentation along with a naloxone schematic with clinical signs and appropriate LEK9 dosages is available free at workingdoghq.com. Handlers were also given a laminated copy of a treatment algorithm for suspected opioid overdose in an LEK9 (Figure 1). This document is free and available to download at workingdoghq.com.
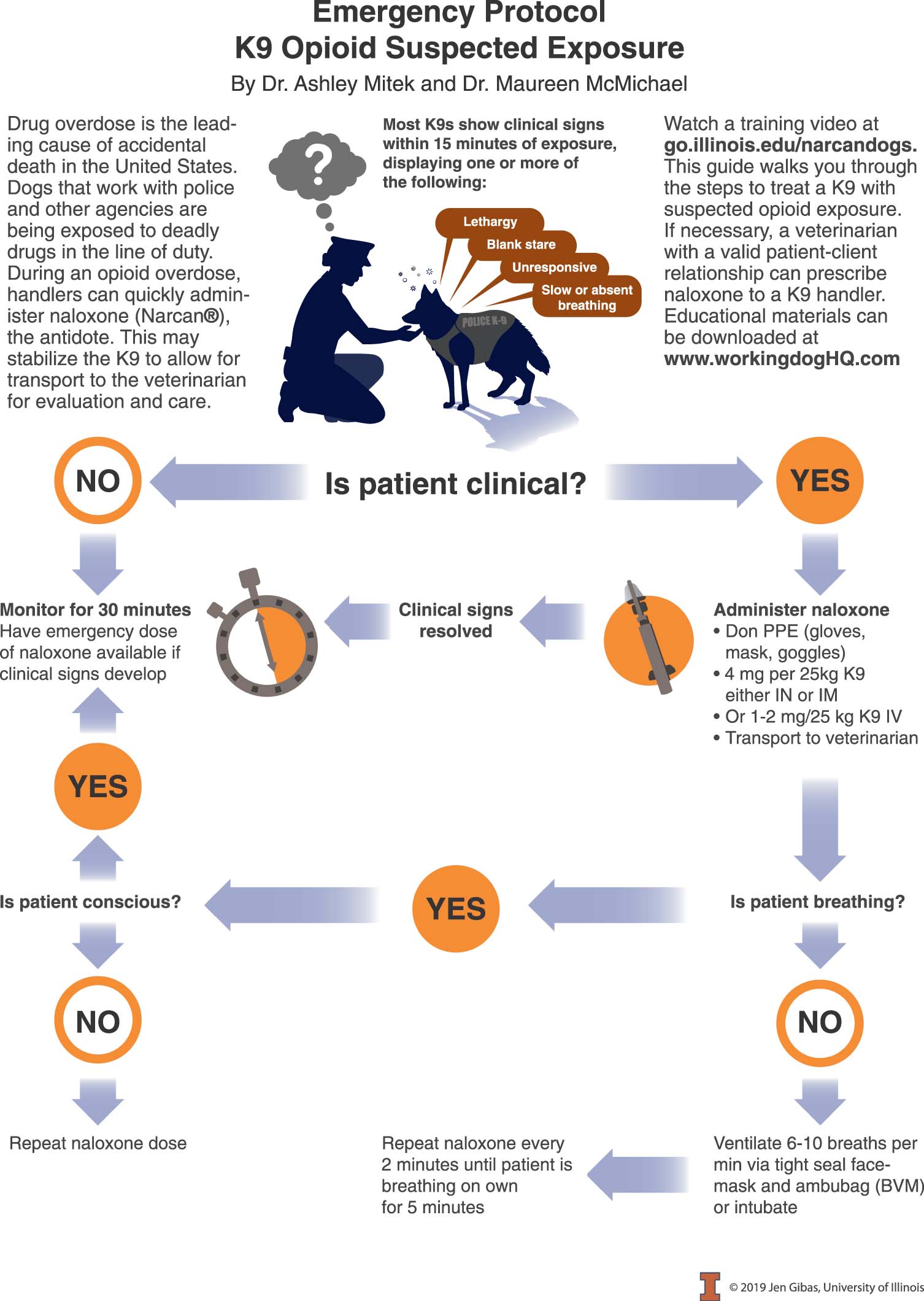
FIGURE 1 Treatment algorithm for suspected K9 opioid overdose. BVM, bag valve mask; IM, intramuscular; IN, intranasal; PPE, personal protective equipment.
Approximately 75 handlers attended the May 2016 LEK9 Handler Training Day. Of those handlers, approximately 50 were part of the agency’s K9 Unit, and others were from other local and state agencies. Institutional review board approval was obtained by the Carle Foundation Hospital Institutional Review Board (protocol #17039).
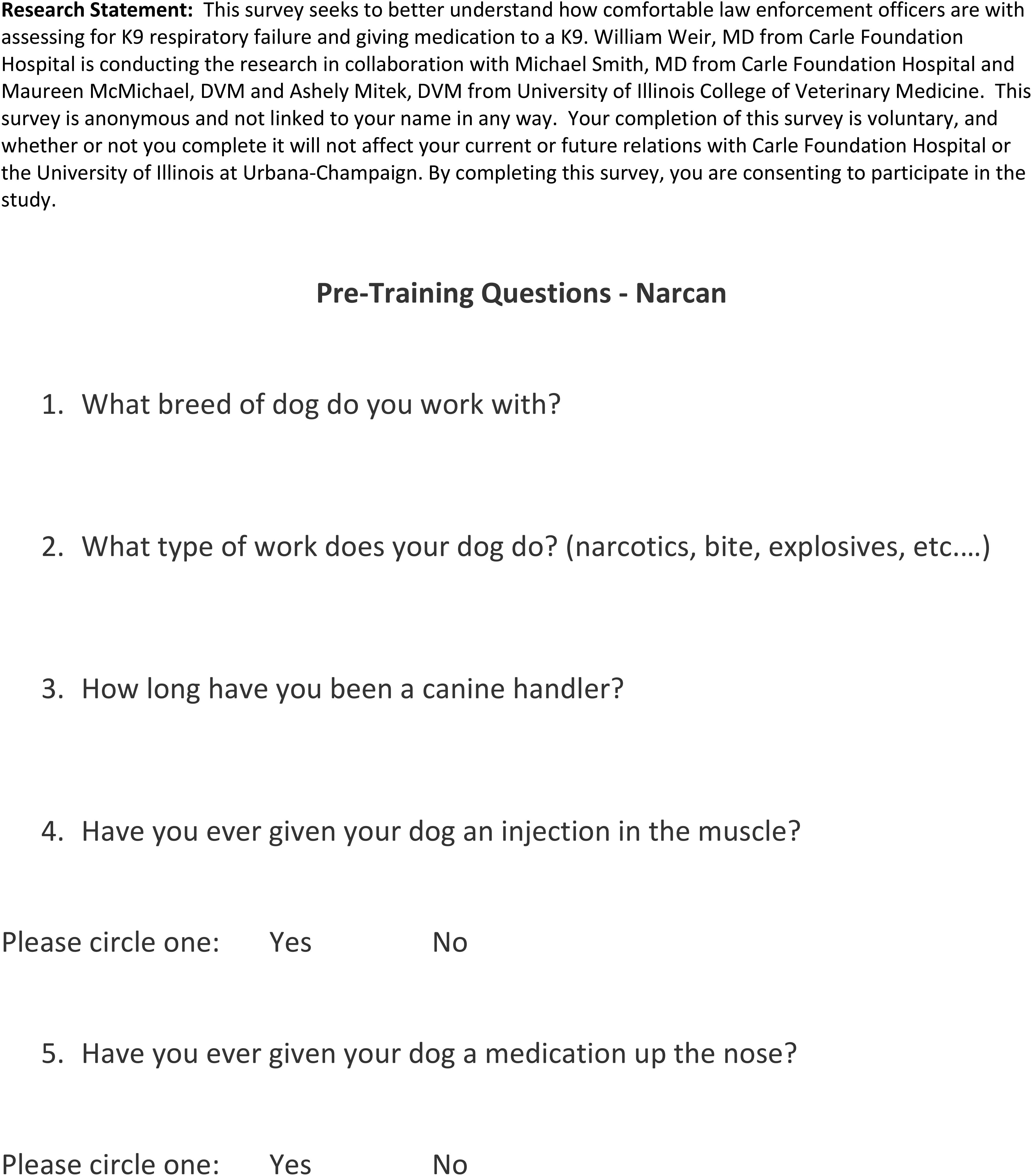
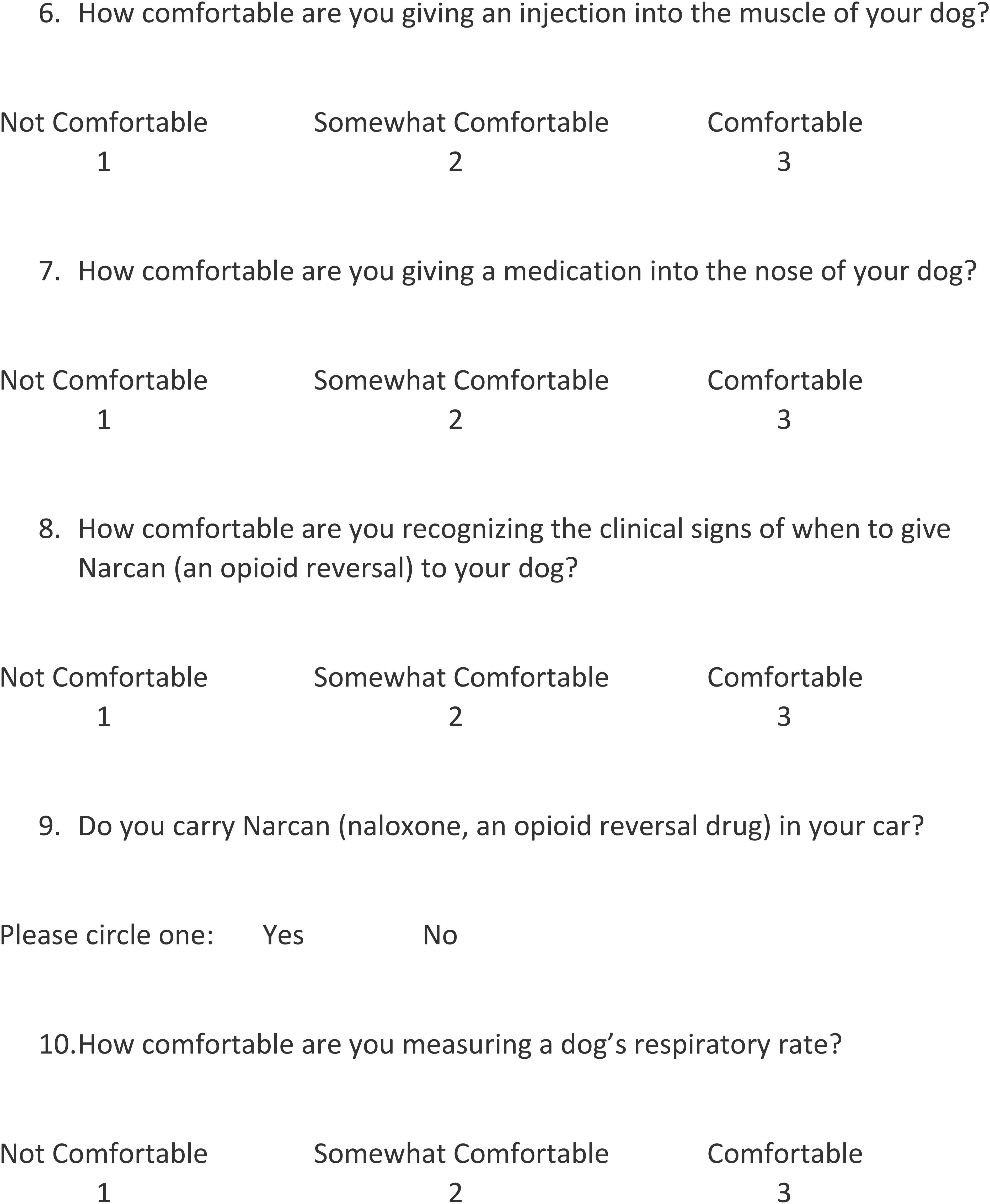
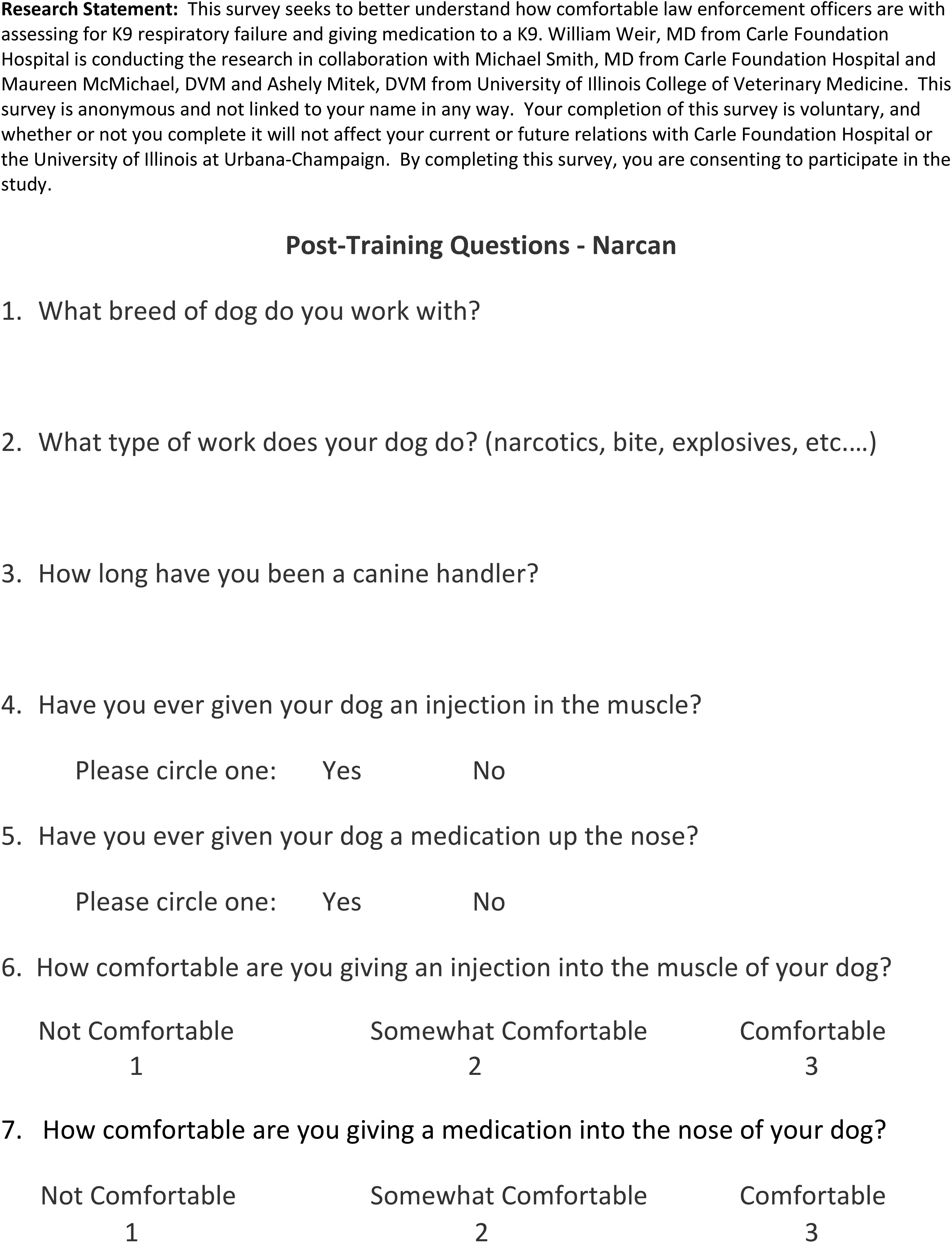
Five minutes before the lecture on naloxone administration, all handlers were given a 10-question prelecture survey (Figure 2). All surveys were anonymous. Three questions pertaining to whether the handler currently carries naloxone and if they have previously given an IM or IN injection to their LEK9 were “Yes” or “No” responses. Three questions pertaining to months of service, breed of LEK9, and type of work were open-ended. The remaining four questions were Likert items based on a 3-point scale evaluating the handler’s comfort administering IN and IM drugs, recognizing opioid overdose symptoms, and monitoring respiratory rate (1 = Not Comfortable, 2 = Somewhat Comfortable, 3 = Comfortable). The handlers anonymously placed the completed presurveys in a sealed envelope. Once all surveys were collected, the 25 min naloxone administration lecture commenced. After the lecture, the handlers completed a postsurvey (Figure 3) to evaluate any change in their knowledge of, and comfort level in, dealing with a future opioid overdose in an LEK9.

Statistics
Surveys were analyzed as simple tables of the number of responses for each score in the Likert item. Exact 1-sided and 2-sided P values were calculated for the difference in the trinomial distributions using StatXact 9.a Exact P values are determined from the fractiles of the trinomial distribution rather than using the large sample approximation from the normal (Gaussian) distribution. Simple bar charts (not shown) were used to visualize the response distributions.
Results
Sixty-two pretraining surveys were completed. Average handler service was 45 mo (3.75 yr). Fifty-two percent of handlers had Belgian Malinois, 15% German shepherd dogs, 15% German shepherd–Malinois mixed-breed dogs, 13% Dutch shepherds, and 6% Labrador retrievers. Ninety-seven percent of handlers (60/62 handlers) had dual-purpose LEK9s, and 3% (2/62 handlers) had explosive detection LEK9s.
Ninety-five percent (59/62 handlers) reported that they had never administered an IM injection to their LEK9. Ninety-seven percent (60/62 handlers) reported they had never given an IN medication to their LEK9. Most handlers (89%, 55/62 handlers) reported they currently carry naloxone for human use when on patrol, and 11% (7/62 handlers) did not.
Forty-seven postlecture surveys were completed anonymously. Compared with the prelecture survey, there was a 15% (7/47 handlers) increase in the number of respondents who selected that they feel “comfortable” giving an IM injection. There was a 15% (7/47 handlers) increase in the number of respondents who selected they feel “comfortable” giving an IN medication, compared with the presurvey.
Prelecture survey data indicated that only 29% of handlers felt comfortable monitoring their LEK9’s respiratory rate, and only 27% felt comfortable recognizing the signs of an opioid overdose. There was a 32% increase in respondents who selected they feel “comfortable” recognizing the clinical signs of opioid overdose, and a 38% increase in respondents who selected they feel “comfortable” measuring their LEK9’s respiratory rate, compared with the presurvey.
Response distributions for selected skills in the pre- and postlecture surveys are summarized in Table 1. The table gives the frequency of each Likert score, the cumulative frequency, and the response frequencies transformed to the proportions of total responses in the survey. Differences between Likert scores in the post and presurveys are given by Δ for both the proportion of the score and the cumulative proportions. For example, 18% of prelecture surveys gave a score of 1 for the handler’s Comfort Giving Muscle Injection whereas only 4% of postlecture surveys gave a score of 1 (not comfortable), so the pre–post change was Δ = 4–18% = –14%, meaning that an additional 14% of responders felt “somewhat comfortable” or “comfortable” after the lecture. Conversely, 55% of the prelecture Likert scores were 3 (comfortable) whereas 70% were comfortable after the lecture, so Δ = 70–55% = +15% more responders were comfortable.
There was no correlation between the handler’s length of service and comfort in various circumstances.
TABLE 1 Distribution of Likert Scores Before and After Lecture for Selected Skills
| Skill | Frequency, n (%) | Change in Frequency (%) Post (%) – Pre (%) |
|
| Likert Score | Post (n = 46) | Pre (n = 62) | Δ |
| Comfort giving muscle injection (exact 1-sided P = .035; exact 2-sided P = .066) | |||
| 1 | 2 (4.3) | 11 (17.7) | –14 |
| 2 | 12 (20.1) | 17 (27.4) | –7 |
| 3 | 32 (69.6) | 34 (54.9) | +15 |
| Comfort giving nasal medication (exact 1-sided P = .0389; exact 2-sided P = .078) | |||
| 1 | 0 (0.0) | 1 (1.6) | –2 |
| 2 | 4 (8.7) | 13 (21.0) | –12 |
| 3 | 42 (91.3) | 48 (77.4) | +14 |
| Comfort recognizing clinical signs (exact 1-sided P = .0001867; exact 2-sided P = .00032) | |||
| 1 | 1 (2.2) | 10 (16.1) | –14 |
| 2 | 18 (39.1) | 35 (56.5) | –17 |
| 3 | 27 (56.7) | 17 (27.4) | +32 |
| Comfort measuring RR (exact 1-sided P = 9.993e–005; exact 2-sided P = .00017) | |||
| 1 | 2 (4.3) | 4 (6.5) | –2 |
| 2 | 13 (28.3) | 40 (64.5) | –37 |
| 3 | 31 (67.4) | 18 (29.0) | +38 |
Because the numbers of respondents differ between pre- and postlecture, the change in comfort level for each Likert score is the difference %respondents post – %respondents pre. RR, respiratory rate.
Discussion
LEK9s provide an important service to our national security and community safety. It is important that handlers be educated to recognize K9 opioid overdose and be trained to administer naloxone. To the authors’ knowledge, this is the first study evaluating a pilot training program to teach LEK9 handlers to administer naloxone. Data from this study suggest that prior to the training, at least half of handlers were comfortable administering naloxone to their LEK9. However, their comfort was significantly less in recognizing the signs of an opioid overdose in their LEK9. Results from this pilot study suggest that a single 25 min lecture on opioid overdose in LEK9s may improve a handler’s knowledge and comfort level in treating their LEK9. Several LEOs commented that hands-on-training with IM and IN naloxone would have increased their confidence and competency. Unfortunately, a hands-on training session was not possible during this educational opportunity.
It is likely that we will continue to see an increase in the number of LEK9s used for public safety. In 2017, the Transportation Security Administration doubled the number of scent detection LEK9s patrolling US airports.13 Data from this study suggest that the majority of handlers did not feel comfortable monitoring their LEK9s’ respiratory rate or identifying symptoms of an overdose prior to the training. These facts highlight a need for the veterinary profession to partner with law enforcement agencies to help ensure that handlers feel comfortable monitoring their LEK9s’ vital signs and being vigilant of risks to them.
It should be noted that naloxone is not available to some handlers for their LEK9 in the United States, and there is controversy as to whether a handler could use the human naloxone kit provided to them on their LEK9, if needed. We recommend that all LEK9 handlers have multiple doses of naloxone available to them and that handlers should be trained to use the specific naloxone device (IM and/or IN) that their department uses in order to feel comfortable in an emergency situation.
Study Limitations
Limitations of this study are the small pre- and postlecture participant numbers as well as the reduced number of postlecture survey responses compared with prelecture responses (47 versus 62, respectively, or 75.8%).
There are an estimated 50,000 LEK9s and handlers in the United States.14 Our data are from a select group of LEK9 handlers who primarily partner with dual-purpose LEK9s. Some states have made naloxone available over the counter and also require all first responders to carry naloxone.15 The majority of handlers in this study carried naloxone, although it is possible that handlers in other states may not have access to the drug.
The teaching method used in this study was lecture. This is a passive teaching method that may lead to lower knowledge retention levels compared with active learning.16 Although the handlers overall self-reported an increased comfort level in recognizing and treating their LEK9 in the event of an opioid overdose, we do not know if these self-reported values are reflective of handlers accurately performing the tasks in the field in a high-stress situation. A related limitation is that anonymity caused two issues with the statistical analysis: (1) the postlecture responders are self-selected and there is no way to know from our data how well this group’s responses anticipate those from the self-selected group of nonresponders; and (2) the decreased number of postlecture nonresponders reduces the sensitivity of Δ, which we define as the difference in the distributions of Likert response values in the pre- and postsurveys.
Before and after surveys were not linked with an ID code. Because of this we were unable to identify if people who were more comfortable were more likely to complete the survey.
Conclusion
A passive learning pedagogical technique (e.g., lecture and a flowchart indicating steps to take in a suspected opioid overdose in an LEK9) was evaluated in this study. Data and experience from this study are being used to create hands-on training for future events. This study suggests that handlers could benefit from additional medical education pertaining to treating their LEK9 in the field. We hope this study encourages other veterinarians to collaborate with LEK9 handlers to provide them with the medical information they will need to save the LEK9’s life.
FOOTNOTES
a StatXact 9; Cytel Inc., Cambridge, Massachusetts
REFERENCES
- Hanel RM, Palmer L, Baker J, et al. Best practice recommendations for prehospital veterinary care of dogs and cats. J Vet Emerg Crit Care (San Antonio)2016;26:166–233.
- Bodnar RJ. K9 patrols: physical and psychological deterrence. Am Jails 1990;2:35–8.
- Drug Enforcement Agency. Fentanyl/Carfentanil Alert for Canine Handlers. Unclassified document emailed to K9 handlers in the United States. Drug Enforcement Agency; 2016.
- Palmer LE, Gautier A. Clinical update: the risk of opioid toxicity and naloxone use in operational K9s. J Spec Oper Med 2017;17:86–92.
- Armenian P, Vo KT, Barr-Walker J, et al. Fentanyl, fentanyl analogs and novel synthetic opioids: a comprehensive review. Neuropharmacology 2018;134(pt A):121–32.
- Kukanich B, Clark TP. The history and pharmacology of fentanyl: relevance to a novel, long‐acting transdermal fentanyl solution newly approved for use in dogs. J Vet Pharmacol Ther2012;35:3–19.
- Centers for Disease Control and Prevention. Opioid overdoses treated in emergency Available at: https://www.cdc.gov/vitalsigns/opioid-overdoses/index.html. Accessed August 18, 2018.
- Seth P, Scholl L, Rudd RA, et al. Overdose deaths involving opioids, cocaine, and psychostimulants – United States, 2015-2016. MMWR Morb Mortal Wkly Rep 2018;67:349–58.
- Ray B, O’Donnell D, and Kahre K. Police officer attitudes towards intranasal naloxone training. Drug Alcohol Depend 2015;146:107–10.
- Wagner KD, Bovet LJ, Haynes B, et al. Training lawenforcement to respond to opioid overdose with naloxone: impact on knowledge, attitudes, and interactions with community members. Drug Alcohol Depend2016;165:22–8.
- Fisher R, O'Donnell D, Ray B, et al. Police officers can safely and effectively administer intranasal naloxone. Prehosp Emerg Care2016;20:675–80.
- Mitek A, McMichael M. Training Video on Reversing Opioid Overdose in Dogs. Available at: https://www.youtube.com/watch?v=Al108zZF6nc. Accessed August 20, 2018.
- Sachs A. Don’t mind the wet nose: TSA enlists more dogs to screen passengers. Washington Post. January 21, 2016. Available at: https://www.washingtonpost.com/lifestyle/travel/dont-mind-the-wet-nose-tsa-enlists-more-dogs-to-screen-passengers-for-explosives/2016/01/20/26e11d98-b983-11e5-829c-26ffb874a18d_story.html?noredirect=on&utm_term=.1a986ff019b2. Accessed August 20, 2018.
- Ingraham C. The surprising reason more police dogs are dying in the line of duty. Washington Post. November 20, 2015. Available at: https://www.washingtonpost.com/news/wonk/wp/2015/11/20/the-surprising-reason-more-police-dogs-are-dying-in-the-line-of-duty/?noredirect=on&utm_term=.8d50d5ec3c48. Accessed August 20, 2018.
- Illinois General Assembly. HB0001. Illinois Heroin Crisis Act. Available at: http://www.ilga.gov/legislation/BillStatus.asp?DocNum=1&GAID=13&DocTypeID=HB&SessionID=88&GA=99. Accessed June 7, 2018.
- Freeman S, Eddy SL, McDonough M, et al. Active learning increases student performance in science, engineering, and mathematics. Proc Natl Acad Sci 2014;111:8410–5.