



Acute vs. Chronic Pain
Acute Pain of Known Cause (e.g., Perioperative or Diagnosed, Known Trauma)
The mechanisms driving acute and perioperative pain are closer to nociceptive/inflammatory pain than they are to chronic or maladaptive pain (see call-out box 1), so acute/perioperative pain is easier to manage. Exact protocols and approaches can vary, but to be successful, they must be practical and feasible for the individual practice setting. The basic principles of effective perioperative pain management are as follows:
- Early, preemptive or preventive use of analgesic therapies to optimize preventive therapy. This refers to the use of analgesic therapies prior to the surgical insult, or as early as possible.41,42 This approach has been shown to be of benefit in dogs.5,6
- Use of a multimodal approach. The pain transmission system is complex and has a lot of redundancy, so interrupting the pain pathways using multiple differing approaches is more effective clinically than relying on a single receptor or mechanism.43
- Providing continuous, overlapping analgesia. An analgesic plan should provide overlapping pain relief and include at least the early “at-home” time period.
- Matching the provision of analgesia to the degree (dose) of surgery or trauma. Greater tissue trauma, especially when it includes nerve damage, and more invasive and longer surgeries are generally associated with more pain.31,44,45
Effective and frequent assessment of the pain status of patients is critical both for the effective management of the individual patient and for evaluating practice protocols. Patients should be assessed preoperatively and at regular intervals postoperatively (e.g., hourly or as appropriate for the status of the patient). Follow-up with owners should be at least daily for the first few days and include standard questions. When feasible, review of owner-captured video is useful.

Diagram illustrating descriptors used to refer to different types of pain. Pain is often classified as either acute or chronic. Arbitrarily, pain of more than 3 months’ duration has been considered chronic. However, there is nothing that suddenly changes after 3 months to create “chronic” pain. The mechanistic drivers of pain likely change on a continuum from acute nociceptive through to the pathological pain states. Acute pain is generally associated with tissue damage or the threat of this and serves the vital purpose of rapidly altering the animal’s behavior to avoid or minimize damage and to optimize the conditions in which healing can take place. Nociceptive and inflammatory pain are usually considered subtypes of acute or adaptive pain. Pain of a longer duration can result in changes in the pain transmission system at multiple levels. Such changes generally facilitate and amplify pain. These changes result in a progressive disconnect between the peripheral lesion and the pain being perceived and, as such, are often described as a “maladaptive” or “pathological” pain state. Neuropathic pain (from direct damage to the nervous system) and functional pain (altered functioning of the pain transmission system) are considered subtypes of chronic or maladaptive pain. When considering this classification system, the reader will realize that clinical pain is often a mixture of all these “types” of pain. The longer the pain state has been going on, the more likely there is to be maladaptive pain present and the more difficult pain is to treat.
Chronic Pain
The practice team’s approach to treating chronic pain depends on the underlying cause of pain, duration, and previous treatment. The guiding principles for the effective management of chronic pain are as follows:
- Assessment, recognition, and acknowledgment of chronic pain. The practice team should employ checklists, clinical metrology instruments, and physical examinations to determine if chronic pain is present.
- Use of a multimodal (combination therapy) approach. Chronic pain involves multiple and often complex changes in the sensory system. 46 A combination of effective, known analgesics and nondrug therapies, combined with appropriate adjunctive therapies, is optimal.
- Prioritization of known efficacious therapeutic modalities.
- Consider the burden of care on the owner (e.g., oral medication of cats, multiple visits to the clinic for therapy).
- Regular reassessment and adaptation of the management regimen. The pain-sensing (nociceptive) system is bidirectionally plastic; that is, with effective pain management, the nociceptive system can return to normal. This means there is less pain to be managed, and the pain management approach can be reduced and simplified.
Using a Decision Tree for Pain Management Therapies
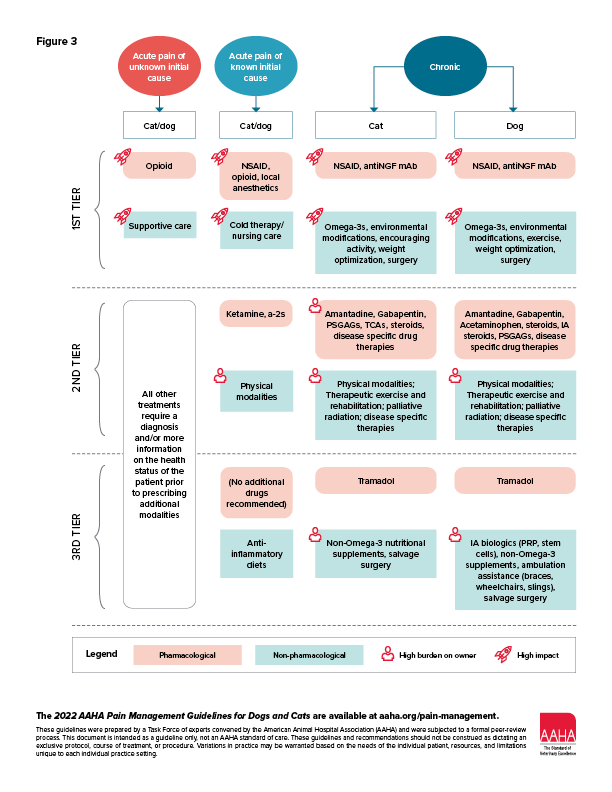
Rather than present a list, or buffet, of treatment options, a tiered decision tree (Figure 3) has been provided to help with prioritizing use of the most efficacious therapeutic modalities. The tiered or ranked approach is based upon review of evidence-based veterinary medicine, incorporation of pertinent literature from human medicine, practical considerations, and clinical experience of the advisory panel. Tier 1 treatments are those that are considered the mainstay of pain management in the respective categories. As further clinical research is performed and new products are developed, the recommendations in each tier will be adapted. Clinicians may choose to start with tier 2 treatments, especially in combination with tier 1 approaches. Treatments in different tiers can be initiated at the same time, for example, NSAIDs and therapeutic exercise for canine OA pain.
Decision Tree for Prioritizing Pain Management Therapies. This figure outlines a tiered approach to pain management in cats and dogs for acute and chronic pain. Tiers are presented from highest recommendation (most evidence for effectiveness) to lowest, although all therapies presented have some evidence to support their use. Physical modalities include laser therapy, pulsed electromagnetic field therapy, acupuncture, and transcutaneous electrical nerve stimulation. Surgical procedures for chronic pain include top-tier treatments such as dental procedures, removal of painful lesions, joint stabilization and replacement, and amputation; lower-tier (salvage) procedures including arthrodesis, denervation, and excision arthroplasty. Anti-NGF mAB, anti–nerve growth factor monoclonal antibody.
Acute Pain of Unknown Cause
In cases in which obvious pain is present but a diagnosis or reason for the pain has not yet been determined, effective management of that pain can facilitate management of the patient. Opioids are considered appropriate in that situation.
Acute Pain of Known Cause (e.g., Perioperative Pain)
An appropriate starting point for every surgery is to plan on using opioids, an NSAID, and local anesthetics, in addition to cold therapy47 and appropriate nursing care.48,49 Local anesthetics are the most effective analgesic available in small animal practice, and they should be used in every surgery. Recently, there has been an increase in information available on the practical use of local anesthetics in practice.50–53 NSAIDs may not be appropriate for every patient, and consideration needs to be given to whether they are provided prior to or after surgery.54,55 Opioids are very effective for perioperative pain56 and have proven preemptive benefit.5 Cold therapy is very effective and can be applied by owners.47 Nursing care includes appropriate use of bandages (which may mean not using them in cats), care of IV lines and other invasive monitoring, gentle massage and range of motion exercise where appropriate, and ensuring animals are able to sleep. Ketamine and a2-adrenoceptor agonists are good analgesic drugs but are in tier 2 to indicate that in general, they should be used after the use of NSAIDs, opioids, and local anesthetics has been considered. There is relatively little in the way of therapeutics with a novel mechanism of action on the horizon for perioperative pain control, but the use of transient receptor potential cation channel subfamily V member 1 (TRPV1) agonists (e.g., capsaicin) holds some promise as a novel approach to augmenting perioperative pain management.57,58
Although there is currently limited evidence of efficacy of physical modalities (laser therapy,59 pulsed electromagnetic field therapy60), future work may change recommendations. Tier 3 contains additional options, including the use of antiinflammatory diets rich in omega-3 fatty acids prior to and after surgery. 61 The tiered approach should be applied to the preoperative, intraoperative, immediate postoperative, and at-home time periods (Figure 3).
Chronic Pain
Dozens of treatments have been suggested as being effective for chronic pain, but there is little evidence of efficacy for the majority of these. The tiered approach attempts to provide a ranking and is based primarily on the management of chronic musculoskeletal pain. However, the principles are generally applicable across other chronic pain conditions. Future work will allow disease- or condition-specific recommendations to be made.
In tier 1 are the COX-inhibiting and non–COX-inhibiting (EP4 receptor antagonist) NSAIDs. These are predictably efficacious across the wide range of pain conditions because of the ubiquitous role of prostaglandins in peripheral and central pain processing. Other analgesics, such as the anti–nerve growth factor (NGF) monoclonal antibodies, are on the horizon and will provide additional first-line choices.62,63 Nondrug treatment options in tier 1 include omega-3 fatty acids (either supplementing the diet or provided through the use of a therapeutic diet), encouraging activity, environmental modification, weight management, and surgery. Measurable pain relief has been associated with the provision of diets enriched in omega-3 fatty acids.64,65 Robust data in humans66,67 and the limited data in companion animals68 support the analgesic benefits of moderate exercise. Modifying the environment is a very practical way of providing relief from painful activities and facilitating movement. Preserving access to 3-D (vertical) space through building ramps or stairs is especially important for cats, who need access to height to feel safe. Lowering entry to litter boxes for cats, providing easy access to elimination for dogs, and optimizing floor and sleeping surfaces are other important aspects. Surgery is listed in tier 1 because particular surgeries can remove chronically painful lesions (cancer resections, dental procedures, joint stabilizations, and amputations).
In tier 2 are adjunctive drugs—those with little or mixed evidence of analgesic efficacy in various conditions. These are recommended as “adjunctive,” or in addition to tier 1 approaches.
In cases of intolerance or contraindications for NSAID use, steroids (cats and dogs) or acetaminophen (dogs only) can be tried as broad “base” analgesics, despite the lack of data.
Intra-articular (IA) steroids are recommended in tier 2, and various IA biologics (such as platelet-rich plasma and stem cells) in tier 3, based on current data. IA treatments are less practical in cats than in dogs. Some pain conditions in cats (e.g., interstitial cystitis) may benefit from tricyclic antidepressants.69 Disease-specific drug and other therapeutic therapies (e.g., bisphosphonates and palliative radiation for osteosarcoma pain) should be considered in tier 2 as appropriate for the disease. Therapeutic exercise and physical modalities such as acupuncture, laser therapy, transcutaneous electrical nerve stimulation, and pulsed electromagnetic field therapy may be useful adjuncts to consider, but little work has been performed to evaluate their benefit in chronic pain.
Tramadol is listed in tier 3 given the demonstrated lack of efficacy in dogs33 and the strong aversion cats have to its taste, despite a potential therapeutic effect.70,71 The placement of nutritional supplements in tier 3 indicates that there is no evidence to support an analgesic effect of non–omega-3 nutritional supplements.72 Procedures such as localized surgical denervation should be considered end-stage procedures.
* These guidelines are supported by generous educational grants from Arthrex Vet Systems, Boehringer Ingelheim Animal Health USA Inc., Elanco, and Zoetis.



