



Chemotherapy Extravasation Management
Extravasation is a term that describes a drug inadvertently or accidentally leaking into surrounding tissue or the subcutaneous space during IV infusions. The volume, contact time, and drug properties are all factors that have to be considered when assessing an extravasation event. Chemotherapeutic agents are at highest risk for complications due to the nature of the agents and the potential to cause high cellular damage when extravasated. The severity of tissue damage can be limited by quick detection of extravasations and swift treatment. A chemotherapeutic extravasation is considered an oncologic emergency.
When assessing a chemotherapy extravasation, it is important to understand the classification of the chemotherapeutic agent in terms of its potential to cause cellular damage if extravasated. Chemotherapeutics can be classified into three categories: vesicants, irritants, and non-irritants.
Vesicants can cause pain, edema, and erythema, and potentially lead to blisters and tissue necrosis when extravasated. Irritants have been described in human medicine as a burning sensation, pain, and/or erythema during injection and extravasation. Non-irritants do not usually produce local reactions to surrounding tissue; however, mild inflammation has been reported. Among veterinary patients, careful monitoring of the patient and injection site for manifestations of erythema and drug leakage during an injection/ infusion would be prudent practice.
Unfortunately at this time, there is not a consensus concerning the management of chemotherapy extravasation in human medicine. Despite a large amount of published literature on this topic, most recommendations are based upon empirical, or anecdotal, evidence. The lack of strength and large variability in management practices in case reports make it difficult to standardize and rank management practice in terms of efficacy. Consequently, this toolkit serves only as a guide for potential treatment options.
Many chemotherapeutic agents do not have known antidotes that are safe to use in order to neutralize their toxic activity. The algorithm on the opposite page should aid in the decision-making process when handling a chemotherapeutic extravasation. It is important to note that the first goal of treatment is to immediately either localize the extravasated agent or disperse the agent. The choice of localization or dispersion depends on the chemotherapeutic agents. Cold compress will help to constrict local blood vessels and localize tissue damage. Warm compress will act in the opposite, aiding to disperse the chemotherapeutic into surrounding tissues. The second goal of treatment is to neutralize the chemotherapeutic once localized or dilute the agent to allow it to be absorbed and consequently metabolized.
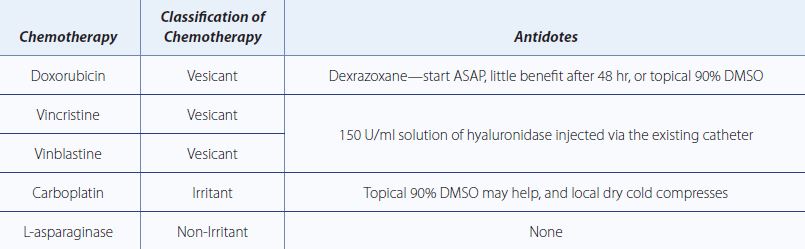
For the purposes of this document, we will focus upon five commonly used chemotherapeutics and their antidotes: doxorubicin, vincristine, vinblastine, carboplatin, and L-asparaginase.
TABLE 1. MANAGEMENT OF EXTRAVASATION
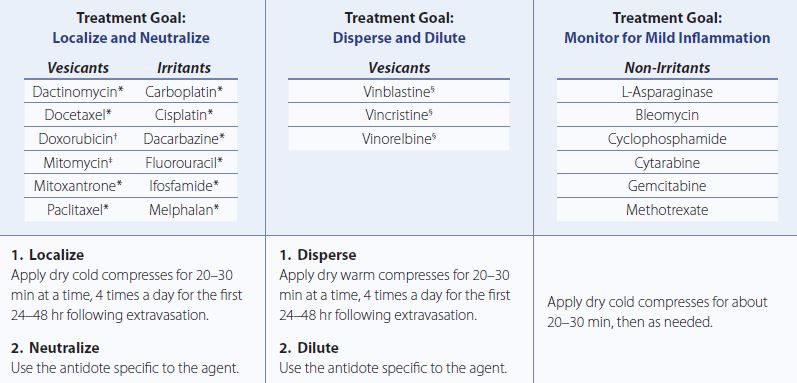
*No recommended antidote. †Recommended antidote: dexrazoxane or dimethyl sulfoxide (DMSO). ‡Recommended antidote: DMSO. §Recommended antidote: hyaluronidase. Adapted from [1].
Anthracycline Extravasations
Doxorubicin Antidotes
Dexrazoxane
Dexrazoxane is an iron chelator that prevents anthracycline-iron complexes and free radical formation causing oxidative damage. Furthermore, dexrazoxane has a protective effect on healthy tissue by stabilizing topoisomerase II, thereby preventing damage from anthracycline. This mechanism of action is responsible for its ability to reduce the cardiotoxicity associated with anthracyclines, such as doxorubicin. Dexrazoxane has the most evidence to support its use in human medicine. In two single arm trials among 54 human patients with anthracycline extravasations, dexrazoxane was shown to be effective in preventing severe tissue damage. Dexrazoxane was administered IV in a three-day schedule (1000, 1000, and 500 mg/m2 on respective days) starting no later than 6 hr after the extravasation event [2]. In mouse models dexrazoxane has been shown to have protective effects against extravasations 3 hr after extravasations [3].
In veterinary medicine, Venable et al. described four case reports in dogs with doxorubicin extravasation; three dogs received varying doses of dexrazoxane within 2 hr of extravasation and 1 after 48 hr. The dogs that received dexrazoxane within 2 hr made full recoveries with no surgical debridement, whereas the dog that received dexrazoxane 48 hr after the event required surgical debridement. Doses varied from 231 to 500 mg/m2 with some varying number of doses given [4].
Dimethyl sulfoxide (DMSO)
DMSO has been used with success in human anthracycline extravasation. In humans, topical DMSO was applied immediately after extravasation covering twice the area affected. This treatment was repeated twice daily for 14 days with resolution [1]. It is important to note that concomitant use of DMSO and dexrazoxane is not recommended and has been shown, in mice, to decrease dexrazoxane efficacy [5, 6]. However, in a case report of 4 dogs with doxorubicin extravasation, all dogs received dexrazoxane along with topical 90% DMSO ointment every 8 hr for 14 days; only 1 dog required surgical debridement but all survived with medical management [4]. Evidence to support DMSO use for doxorubicin extravasation exists; however, the strength and variability of that data do not support DMSO’s use as first-line treatment of doxorubicin extravasation.
Vinca Alkaloid Extravasations
Vincristine and Vinblastine Antidotes
Hyaluronidase
Hyaluronidase is an enzyme that degrades hyaluronic acid, improving the absorption of the extravasated drugs into circulation where they can be metabolized [1]. A study with seven human patients with accidental vinca alkaloid extravasation showed no skin necrosis after local treatment with hyaluronidase [7]. Data from this study showed use of a 150 U/ml solution of hyaluronidase injected through the existing catheter line was beneficial. The dose was 1:1, 1 ml hyaluronidase (150 U/ml) for every 1 ml of extravasated drug. Warm compresses help disperse vinca alkaloids, which helps minimize vesicant toxicity.
Alkylating Agents
Carboplatin
DMSO
Application of topical DMSO over the affected skin surface every 8 hr for 1 wk along with a local dry cold compress have been shown to be beneficial in humans [8]. Medical management with antihistamines or anti-inflammatories may be beneficial if needed.
L-Asparaginase
As L-asparaginase is a non-irritant, it is fairly benign. Local dry cold compresses will help with any reactions [1].
SUMMARY OF CHEMOTHERAPEUTIC ANTIDOTES
References
- Fidalgo JA, Pérez L, García Fabregat A, et al. Management of chemotherapy extravasation: ESMO-EONS Clinical Practice Guidelines. Ann Oncol 2012; 23 (Supplement 7): vii167–vii173. Oxford University Press. http://annonc.oxfordjournals.org/content/23/suppl_7/vii167.full.pdf. Accessed Mar 3 2015.
- Mouridsen HT, Langer SW, Buter J, et al. Treatment of anthracycline extravasation with savene (dexrazoxane): results from two prospective clinical multicenter studies. Ann Oncol 2007; 18: 546–550.
- Langer SW, Sehested M, Jensen PB. Treatment of anthracycline extravasation with dexrazoxane. Clin Cancer Res 2000; 6: 3680–3686.
- Venable RO, Saba CF, Endicott MM, et al. Dexrazoxane treatment of doxorubicin extravasation injury in four dogs. Journal of the American Veterinary Medical Association 2012; 240(3): 304-07.
- Langer SW. Extravasation of chemotherapy. Curr Oncol Rep 2010; 12(4):242–246. doi: 10.1007/s11912-010-0110-7.
- Langer SW, Thougaard AV, Sehested M, Jensen PB. Treatment of anthracycline extravasation in mice with dexrazoxane with or without DMSO and hydrocortisone. Cancer Chemother Pharmacol 2006; 57(1):125–128. doi: 10.1007/s00280-005-0022-7.
- Bertelli G, Dini D, Forno GB, et al. Hyaluronidase as an antidote to extravasation of vinca alkaloids: clinical results. J Cancer Res Clin Oncol 1994; 120: 505–506.
- Bertelli G, Gozza A, Forno GB, et al. Topical dimethylsulfoxide for the prevention of soft tissue injury After extravasation of vesicant cytotoxic drugs: a prospective clinical study. J Clin Oncol 1995; 13: 2851–2855.