



Categorical Approach to Diagnosis Based on Clinical Presentation
In the past, patients have been diagnosed with CS based on classic clinical signs (polyuria, polydipsia, polyphagia, panting, and dermatologic abnormalities), clinicopathologic abnormalities (increased ALP and cholesterol, stress leukogram, thrombocytosis, urine specific gravity <1.020, and proteinuria), and definitive diagnostics (LDDST or ACTHST). However, as awareness of CS has increased, clinical suspicion has also increased in patients with more ambiguous presentations that may lack some of the classic clinical signs or clinicopathologic abnormalities. The purpose of the information in this section of the guidelines is to help the practitioner navigate the diagnostic pathway in patients with various presentations.
TABLE 4
Summary of Categorical Approach to Diagnosing Suspected Canine Hypercortisolism (Cushing’s Syndrome)
Download PDF
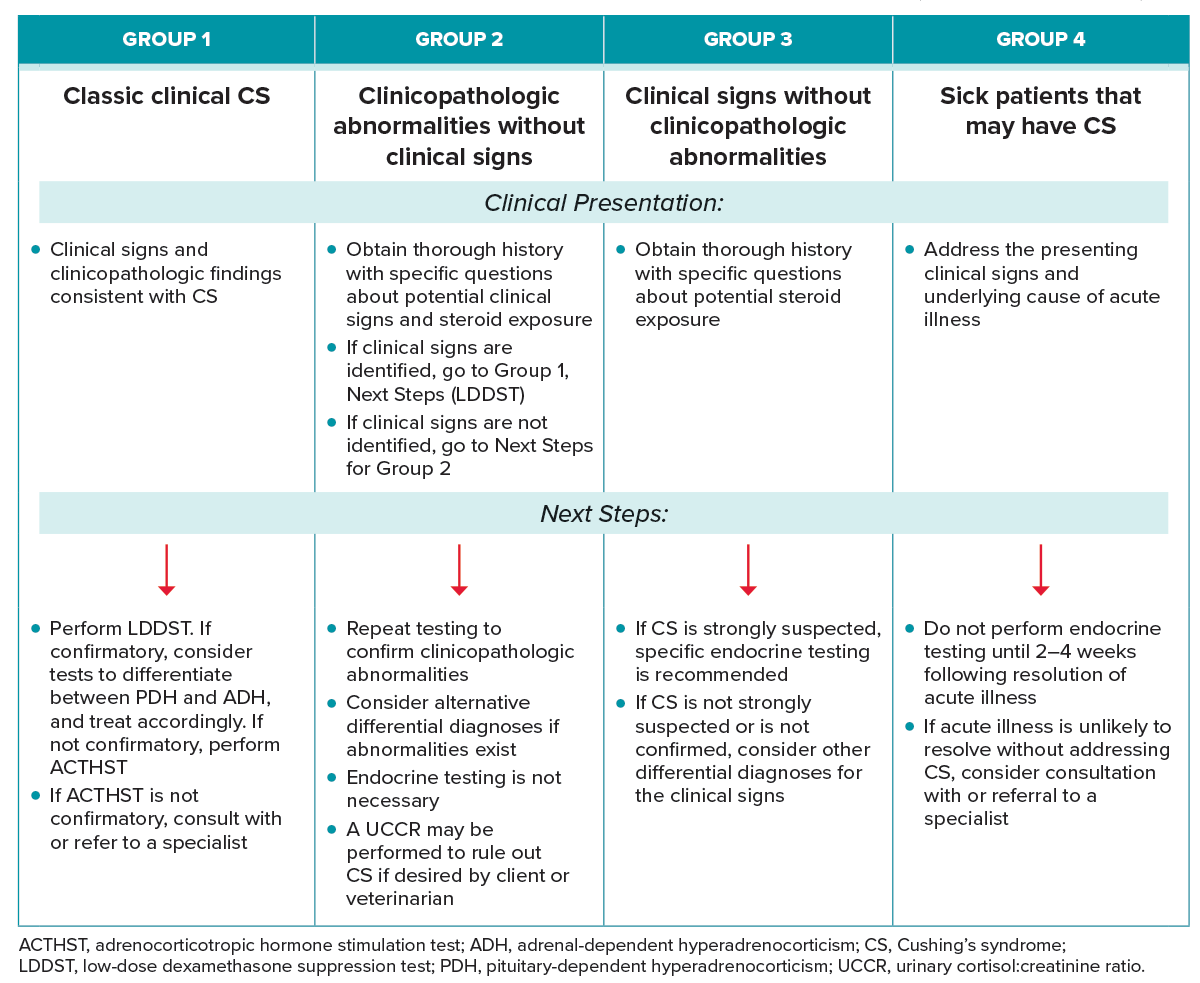
GROUP 1: CLINICAL SIGNS AND CLINICOPATHOLOGIC FINDINGS CONSISTENT WITH CUSHING’S SYNDROME
Clinical presentation
These are the dogs with classic signs and clinicopathologic abnormalities expected with CS (Tables 2 and 3).
Table 2
Clinicopathologic Findings That Can Occur with Cushing’s Syndrome
Download PDF
| Increased alkaline phosphatase |
| Hypercholesterolemia |
| Mild hyperglycemia |
| Dilute urine (specific gravity <1.02 0) |
| Proteinuria |
| Stress leukogram (mature neutrophilia, lymphopenia, eosinopenia, monocytosis) |
| Thrombocytosis |
| Erythrocytosis |
| Systemic hypertension |
TABLE 3
Clinical Signs Associated With Naturally Occurring Cushing’s Syndrome
Download PDF
| Polyuria (± worsened incontinence, urinary accidents, and/or nocturia) |
| Polydipsia |
| Pot-bellied appearance |
| Polyphagia |
| Excessive panting |
| Dermatopathy |
| Muscle weakness or wasting |
Next Steps
- Minimum database should include complete blood count, serum biochemistry, and urinalysis. Consider assessing blood pressure, urine culture, and urine protein:creatinine ratio.
- Specific endocrine testing should be performed. The guidelines panel recommends an LDDST as a routine first step. If the LDDST confirms CS, consider differentiation between PDH and ADH (if not differentiated by the LDDST) and appropriate therapy.
- Differentiation between PDH and ADH is helpful because it helps direct therapeutic options and provides the owner with prognostic information. However, if the owner has no intention of pursuing adrenalectomy if an adrenal tumor is identified, patients can be treated with trilostane without knowing whether the dog has PDH or ADH.
- Diagnostics that help differentiate PDH from ADH include LDDST, abdominal ultrasound, and endogenous ACTH concentration.
- Computed tomography of the head may be performed in dogs with PDH if the dog has signs compatible with a macroadenoma or if the owner would pursue radiation therapy or hypophysectomy.
- In patients with ADH, abdominal computed tomography is usually pursued before adrenalectomy.
- If the LDDST is not confirmatory, perform an ACTHST. If the ACTHST is confirmatory, consider differentiation and therapy. If the ACTHST is not confirmatory, consider referral to a specialist.
- Note that endocrine diagnostics should not be performed within 2 wk of administration of short-acting glucocorticoids (oral, otic, or ophthalmic) or within 4 wk of receiving long-acting glucocorticoids.33–35
GROUP 2: DOGS WITH NO CLINICAL SIGNS, BUT WITH CLINICOPATHOLOGIC ABNORMALITIES SUGGESTIVE OF CUSHING’S SYNDROME
Clinical presentation
Group 2 dogs are those for whom the owners report no clinical signs consistent with CS but have one or more compatible clinicopathologic abnormalities (Table 2).
Next Steps
- The first step in managing these patients is to thoroughly probe the patient’s history, with specific questions about water intake, urination habits, worsened incontinence, or nocturia. Potential administration of glucocorticoids, including ophthalmic or otic preparations, should also be ruled out.
- Repeat testing to confirm persistence of previous abnormalities.
- If no clinical signs of CS are identified, consider alternative differentials for clinicopathologic abnormalities, and pursue appropriate diagnostics. For example, for an increased ALP concentration, abdominal imaging may be performed.
- Specific endocrine testing is not necessary unless or until clinical signs of CS are present.
- A UCCR test may be considered if the veterinarian or client is highly motivated to rule out the diagnosis of CS. Note that the UCCR test is a very sensitive but nonspecific test. Although a negative result makes CS very unlikely, a positive result does not confirm the presence of CS.
GROUP 3: DOGS WITH CLINICAL SIGNS SUGGESTIVE OF CUSHING’S SYNDROME WITHOUT CLINICOPATHOLOGIC ABNORMALITIES
Clinical presentation
Clinical signs in Group 3 dogs may include polyuria, polydipsia, polyphagia, excessive panting, and dermatopathy (Table 3).
Next Steps
- Carefully question the owner to rule out administration of glucocorticoids that could cause CS.
- If clinical suspicion of CS is low, monitor the patient’s progression or change in clinical signs. A UCCR test can be considered to rule out CS.
- If clinical suspicion is high, specific endocrine testing is recommended. In patients without significant comorbidities (such as diabetes mellitus), an LDDST is recommended.
- If CS is confirmed, consider differentiation (see GROUP 1). If CS is not confirmed, consider other differential diagnoses for the specific clinical signs.
- If CS is still strongly suspected, ACTHST and/or consultation with a specialist may be pursued.
GROUP 4: SICK PATIENTS PRESENTING WITH SIGNS AND/OR CLINICOPATHOLOGIC FINDINGS CONSISTENT WITH CUSHING’S SYNDROME
Clinical presentation
Group 4 dogs are patients that may have CS but whose presenting signs must be addressed before pursuing diagnostics for CS. Note that hypercortisolism does not cause anorexia, vomiting, or diarrhea. Patients in this category may include:
- Dogs in whom the presenting signs are due to a disease process that is unrelated to CS (e.g., acute gastroenteritis)
- Dogs with presenting signs caused by a comorbidity associated with CS (e.g., pulmonary thromboembolism, gall bladder mucocele, or diabetic ketoacidosis)
- Dogs with signs of an enlarging macroadenoma (decreased appetite, behavior change, or other neurologic signs). In these cases, the macroadenoma is causing the presenting signs; hypercortisolism is not.
Next Steps
- Address the presenting clinical signs and underlying cause of the acute illness.
- Do not perform specific endocrine testing for CS until the acute illness is managed or controlled. Acute illness causes stress that can lead to false-positive results, particularly with the LDDST. Additionally, because CS is not causing the presenting clinical signs, diagnosis and treatment of CS will not immediately ameliorate the presenting clinical signs.
- If relevant, treatment of diabetes mellitus should not be delayed in dogs with suspected CS.
- The guidelines task force recommends, if possible, waiting at least 2–4 wk after improvement of the acute illness to test for CS.
- If the acute or chronic illness is unlikely to resolve or improve without addressing the possible underlying CS, consider consultation with a specialist to discuss the need for and timing of specific endocrine testing.
The 2023 AAHA Selected Endocrinopathies of Dogs and Cats Guidelines are generously supported by Boehringer Ingelheim Animal Health, IDEXX, Merck, Zoetis, and Zomedica.



