



Categorical Approach to Diagnosis Based on Clinical Presentation*
TABLE 9
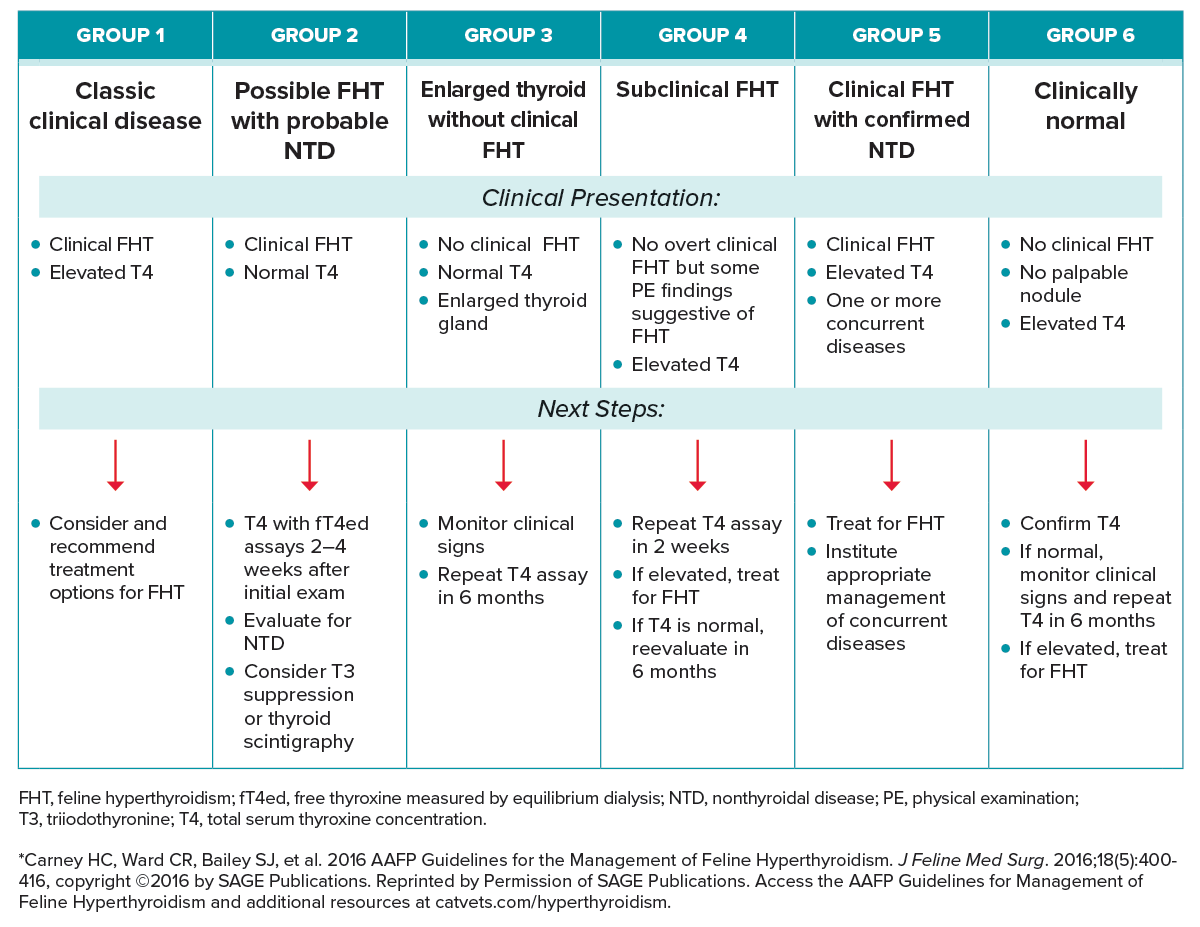
Summary of Categorical Approach to Diagnosing Suspected Feline Hyperthyroidism
Download PDF
Important Note
The AAHA guidelines task force recommends for AAFP groups 4 and 6, the practitioner should consider checking TSH prior to 131I treatment and postponing if measurable (>0.03 ng/mL) to help avoid creating iatrogenic hypothyroidism.70
GROUP 1: CLASSIC CLINICAL DISEASE
Clinical Presentation
Cats with uncomplicated clinical hyperthyroidism and elevated T4. These are cats with one or more clinical signs consistent with FHT that have an elevated T4 and no identifiable concurrent disease. T4 is above the laboratory reference interval in FHT cases.
Next Steps
The AAFP Guidelines Panel recommends that reference laboratory testing be utilized for diagnosis and monitoring of FHT so that precise serum hormone levels can be followed throughout treatment and to avoid quality control discrepancies. Ideally, for purposes of consistency, monitoring should be performed at the same reference laboratory. If in-clinic testing is performed for geriatric screening and significant changes are noted in thyroid hormone levels, obtain confirmatory testing at a reference laboratory.
Complete blood count (CBC) findings are generally unremarkable, although macrocytosis may be present. Cats with marked anemia may suffer from a comorbidity and further work-up should be performed. Serum chemistry findings often include elevated serum alanine transferase (ALT) or alkaline phosphatase. Serum ALT levels can be markedly elevated.
If liver enzymes do not normalize after successful treatment for FHT, further diagnostic work-up is warranted. Azotemia may suggest dehydration or underlying renal failure. Urinalysis results are variable, although the urine specific gravity may be less than 1.030 due to primary polydipsia or inability to concentrate the urine due to hyperthyroidism.
Management of Group 1 cats consists of treatment for their hyperthyroid disease.
GROUP 2: POSSIBLE FHT WITH PROBABLE NON-THYROIDAL DISEASE
Clinical Presentation
Cats with clinical hyperthyroidism and normal T4. Cats in this category have clinical signs suggestive of FHT along with T4 within the laboratory reference interval.
Next Steps
The AAFP Guidelines Panel recommends the following approaches for Group 2 cats:
- Further testing for FHT should consist of T4 and fT4 assays measured 2–4 weeks after the initial blood screening. A T4 value in the upper half of the reference interval combined with an elevated fT4 supports a diagnosis of hyperthyroidism.
- If the T4 and fT4 are both within the reference interval, the cat should be evaluated for non-thyroidal disease.
- If no concurrent illness is found and FHT is still suspected, further testing is warranted, including triiodothyronine (T3) suppression testing, serum TSH concentration in conjunction with T4 and fT4ed, or thyroid scintigraphy.
NOTE: Common conditions with signs similar to FHT: Certain classic signs of hyperthyroidism (polydipsia, polyuria, weight loss in the face of a good appetite) have similarities with the following morbidities that are plausible differential diagnoses:
- Diabetes mellitus
- Gastrointestinal malabsorption, maldigestion
- Gastrointestinal neoplasia, especially lymphosarcoma
GROUP 3: ENLARGED THYROID GLAND WITHOUT CLINICAL FHT
Clinical Presentation
Cats without clinical hyperthyroidism, T4 within the reference interval, but with enlarged thyroid gland(s).
Next Steps
Monitor clinical signs in these cats and repeat a serum T4 assay in 6 months.
GROUP 4: SUBCLINICAL FHT
Clinical Presentation
Cats without overt clinical hyperthyroidism but with an elevated T4 and with some physical exam findings suggestive of hyperthyroidism.
Next Steps
Repeat the T4 test in 1–2 weeks. If serum T4 is still elevated, treat the cat for FHT. While no data exist for the best way to manage Group 4 cats, the consensus of the Panel is to treat these cats for hyperthyroidism. If a repeat T4 is normal, then re-evaluate the patient in 6 months with a complete physical exam and a T4 assay.
GROUP 5: CLINICAL FHT WITH CONFIRMED NON-THYROIDAL DISEASE
Clinical Presentation
Cats with clinical hyperthyroidism confirmed by elevated T4, and one or more concurrent diseases.
Next Steps
Hyperthyroid cats are commonly middle-aged or older and often have concurrent diseases. But because FHT is a serious disease that can result in rapid deterioration of the patient, the Panel recommends the treatment of all diagnosed cats, including those animals with comorbidities. Appropriate monitoring and careful management of concurrent diseases will optimize the patient’s health.
Common comorbidities associated with FHT:
- Thyrotoxic heart disease
- Hypertension
- Retinopathy
- CKD
- Gastrointestinal disease, malabsorption, cobalamin deficiency
- Insulin resistance
GROUP 6: CLINICALLY NORMAL
Clinical Presentation
Cats with no clinical signs of hyperthyroidism and no palpable thyroid nodule but with an elevated T4 on screening lab test.
Next Steps
Because falsely elevated T4 values may occur, repeat the T4 test preferably using radioimmunoassay or chemiluminescent enzyme assay.74,75 If the T4 is now normal, monitor the cat and retest T4 every 6 months, or sooner if clinical signs develop. If the T4 is elevated, treat for FHT.
*Carney HC, Ward CR, Bailey SJ, et al. 2016 AAFP Guidelines for the Management of Feline Hyperthyroidism. J Feline Med Surg. 2016;18(5):400-416, copyright © 2016 by SAGE Publications. Reprinted by Permission of SAGE Publications. Access the AAFP Guidelines for Management of Feline Hyperthyroidism and additional resources at catvets.com/hyperthyroidism.
The 2023 AAHA Selected Endocrinopathies of Dogs and Cats Guidelines are generously supported by Boehringer Ingelheim Animal Health, IDEXX, Merck, Zoetis, and Zomedica.



