



Categorical Approach to Diagnosis Based on Clinical Presentation
Although some dogs with hypoadrenocorticism present with typical physical examination and laboratory abnormalities, making diagnosis relatively straightforward, other cases may have a vague or atypical presentation. The clinical signs or laboratory findings associated with hypoadrenocorticism can mimic several other diseases, making diagnosis challenging. The guidelines panel has organized clinical presentations into four groups to aid in diagnosis.
TABLE 8
Summary of Categorical Approach to Diagnosing Suspected Canine Hypoadrenocorticism
Download PDF
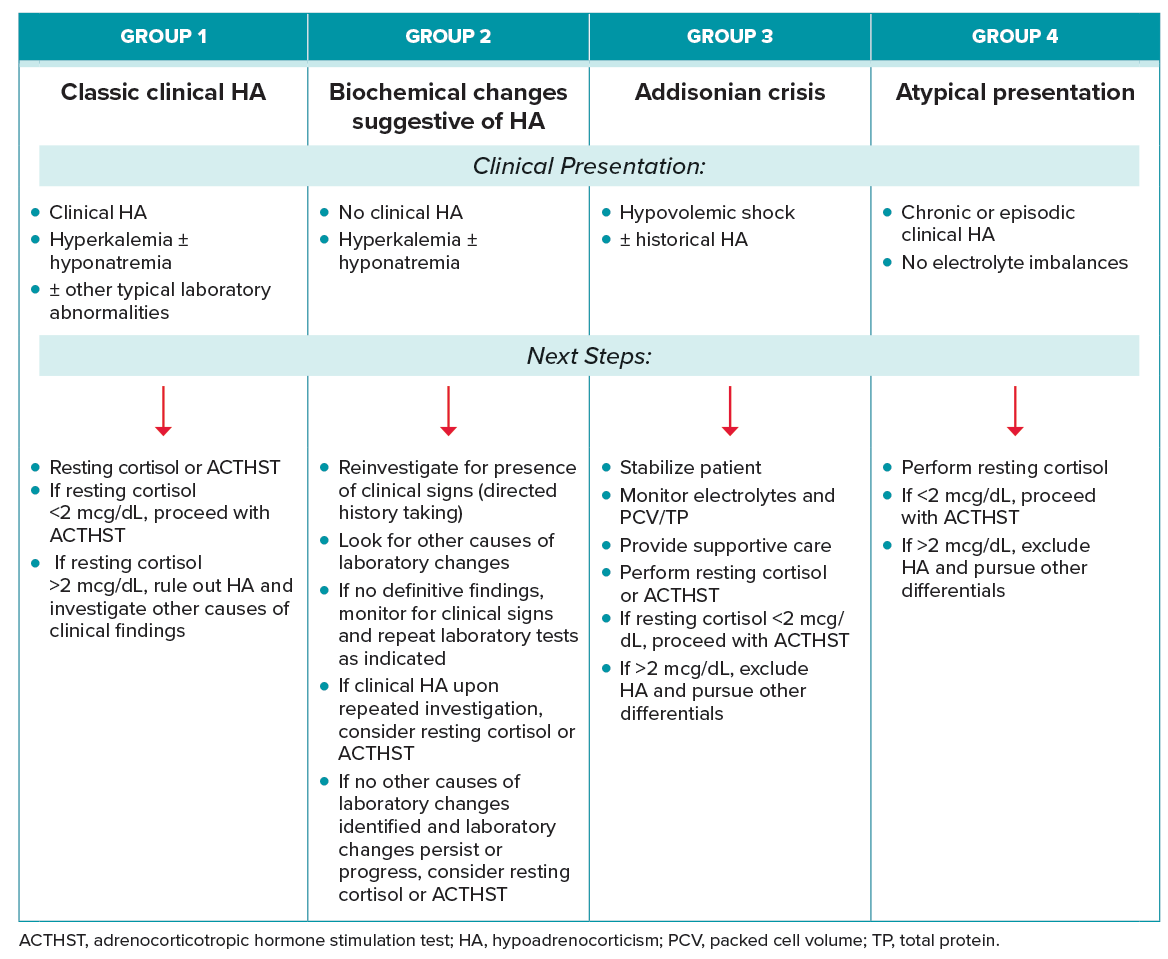
GROUP 1: CLASSIC CLINICAL DISEASE
Clinical Presentation
Group 1 dogs present with chronic or episodic clinical signs and laboratory abnormalities consistent with hypoadrenocorticism.
Next Steps
If suspicion for disease is high, an ACTHST should be performed to confirm diagnosis. If suspicion for disease is low, a resting cortisol could be performed. If the resting cortisol is <2 mcg/dL, an ACTHST should be performed to diagnose hypoadrenocorticism. If the resting cortisol is >2 mcg/dL, other differentials for these clinical and laboratory abnormalities should be pursued.
Once the diagnosis of hypoadrenocorticism is confirmed, appropriate treatment(s) and monitoring should be instituted. For patients with classic clinical disease, treatment generally consists of both mineralocorticoid and glucocorticoid supplementation.
GROUP 2: NO CLINICAL SIGNS, BUT WITH CLASSIC LABORATORY ABNORMALITIES
Clinical Presentation
Group 2 dogs present without clinical signs of disease and have laboratory derangements on routine laboratory work, which include hyperkalemia and/or hyponatremia. Additional laboratory abnormalities may be present (Table 7).
Next Steps
In these cases, the owner should be requestioned as to the presence of associated clinical signs including questions related to gastrointestinal health (appetite and stool), energy, and water intake. If upon deeper analysis there are still no clinical signs of hypoadrenocorticism, other causes of laboratory changes such as spurious causes should be ruled out (Table 6). If the blood sample was run on serum, consider reevaluation of plasma because serum potassium levels can be artificially high due to potassium release from platelets during clot formation.65 If no clinical signs are present and spurious causes have been excluded, monitor clinical signs and repeat the laboratory testing as indicated.
If laboratory abnormalities are persistent or progressive, or upon deeper analysis clinical signs are present, either a resting cortisol should be considered to exclude this disease or an ACTH stimulation test (ACTHST) could be performed.52 If a resting cortisol test is chosen and results are <2 mcg/dL, an ACTHST should be performed to confirm the diagnosis.
GROUP 3: ADDISONIAN CRISIS
Clinical Presentation
Group 3 dogs present in hypovolemic shock with or without historic episodic signs consistent with hypoadrenocorticism. This is the most serious and life-threatening manifestation of hypoadrenocorticism and typically presents as hypovolemic shock accompanied by severe hyperkalemia and hyponatremia. Other laboratory abnormalities may be seen (Table 7).
Next Steps
Immediate stabilization should be implemented, with IV fluids being the cornerstone of therapy. Treatment should target correcting hypovolemia and hypotension. Specific therapy to correct hyperkalemia, hypoglycemia, and acidosis may be required. Gastrointestinal support including early enteral nutrition should be implemented as needed.
Once stable, these patients may need to be transferred to a facility that provides 24 hr care to provide continued support. Frequent monitoring of electrolytes is required. The guidelines task force recommends daily packed cell volume monitoring as these patients can become severely anemic following rehydration.66
Once stable, perform a baseline cortisol test to rule out this diagnosis, or, if suspicion for disease is high, perform an ACTHST to confirm diagnosis. In some cases, administering a single dose of a steroid before testing is required for stabilization. Dexamethasone (0.1 mg/kg IV) is the steroid of choice because it does not interfere with the cortisol assay.66 Consider aldosterone measurement. Mineralocorticoids can be started once the patient is stable, there is a confirmed diagnosis, and sodium is >130 mEq/dL.
GROUP 4: CLINICAL SIGNS WITH NONSPECIFIC LABORATORY ABNORMALITIES (ATYPICAL PRESENTATION)
Clinical Presentation
Group 4 dogs present with chronic or episodic clinical signs without the characteristic findings associated with classic hypoadrenocorticism. Because signs of canine hypoadrenocorticism can mimic many other diseases, patients may present with episodic clinical signs that could be consistent with this disease without the hallmark laboratory findings of hyperkalemia or hyponatremia (Table 6).
Next Steps
When signalment and clinical signs are consistent with hypoadrenocorticism (e.g., episodic gastrointestinal signs after periods of stress, polyuria/polydipsia) or if there are other suggestive laboratory findings (Table 7), a resting cortisol should be performed. If the resting cortisol is <2 mcg/dL, an ACTHST should be performed. If the resting cortisol is >2 mcg/dL, other differentials should be considered. If hypoadrenocorticism is diagnosed, consider testing for aldosterone deficiency as many of these patients have hypoaldosteronism, even with normal electrolytes.51 Appropriate treatment and monitoring should be instituted based on diagnosis.
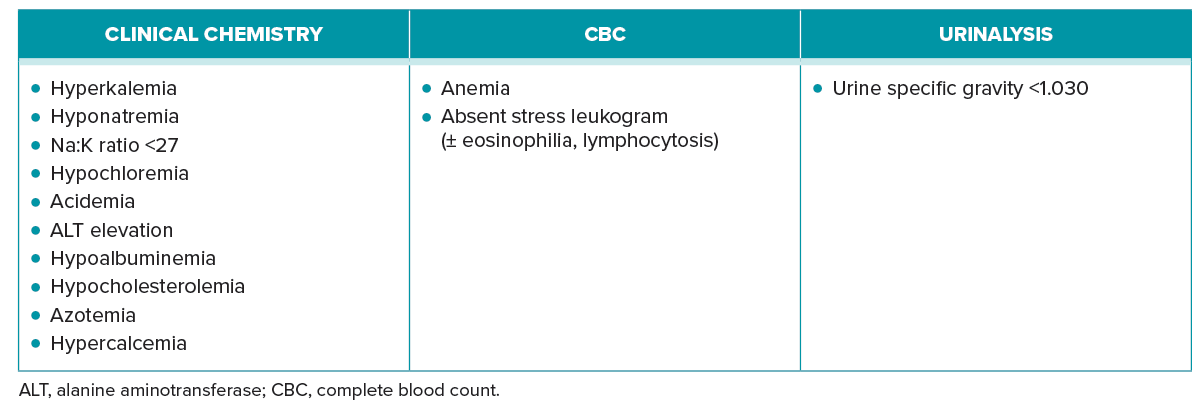
TABLE 7
Laboratory Changes That Can Occur with Hypoadrenocorticism
Download PDF
The 2023 AAHA Selected Endocrinopathies of Dogs and Cats Guidelines are generously supported by Boehringer Ingelheim Animal Health, IDEXX, Merck, Zoetis, and Zomedica.



