



Categorical Approach to Diagnosis Based on Clinical Presentation
Hypothyroidism is one of the most common endocrinopathies of the dog, and a clear-cut diagnosis can be made when the signalment and presentation of symptoms are classic and are supported by appropriate endocrine test results. However, the guidelines authors acknowledge that hypothyroidism is commonly overdiagnosed owing to the nonspecific nature of the signs, as well as the challenges that arise with the interpretation of thyroid function testing.
TABLE 1
Summary of Categorical Approach to Diagnosing Suspected Canine Hypothyroidism
Download PDF
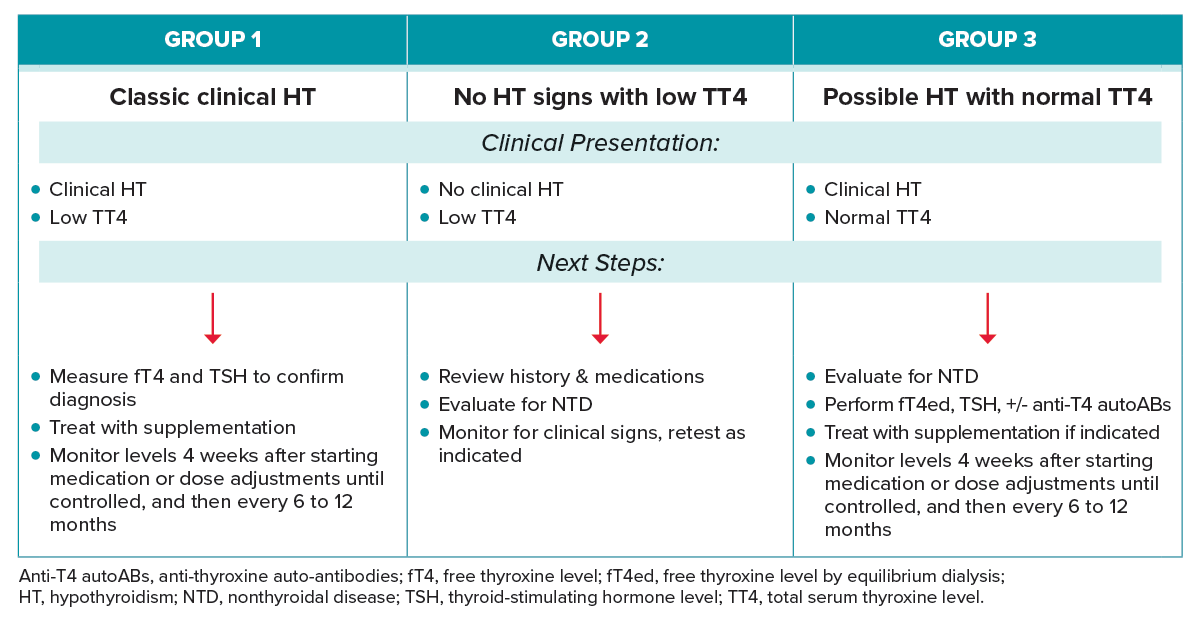
GROUP 1: DOGS WITH CLASSICAL SIGNS OF HYPOTHYROIDISM AND A LOW TT4
Clinical Presentation
- Signalment: middle-aged dogs and breed predisposition (beagles, golden retrievers, Doberman pinschers, Great Danes).13
- Group 1 dogs have one or more signs of hypothyroidism, most commonly including indications of decreased basal metabolic rate (weight gain without historical increase in appetite, cold intolerance or heat seeking, exercise intolerance, lethargy) and dermatological changes (alopecia, seborrhea, dry coat and skin, hyperpigmentation, myxedema, or recurrent pyoderma or otitis externa).
- Other systems that may be affected are cardiovascular (bradycardia) and neurologic, with signs related to the peripheral nervous system (i.e., facial nerve paralysis), vestibular and central nervous systems (ataxia, seizures, obtundation), and polyneuropathy (weakness).7 Megaesophagus has been diagnosed in dogs with hypothyroidism, but there is little evidence of a causative linkage.13
- Assess for consistent laboratory abnormalities such as hypercholesterolemia and hypertriglyceridemia (ideally on a fasted sample). A mild nonregenerative anemia may also be present.
Next Steps
- Submit additional thyroid testing to document a subnormal fT4 and/or an elevated TSH concentration to confirm diagnosis.
- Approximately 20–40% of dogs with hypothyroidism have a low TT4 and low fT4 but a normal TSH concentration.15,16 However, this scenario could also indicate nonthyroidal illness, so additional testing such as assessing for the presence of antithyroid autoantibodies or a TSH response test can be run to help confirm diagnosis, although these tests may be cost-prohibitive for some clients.24
- Initiate treatment with twice-daily levothyroxine supplementation (ideally on an empty stomach to maximize absorption).
- Monitor therapy based on clinical improvement and serial TT4 testing. Assess a TT4 level 4–6 hr post morning pill 4 wk after starting medication or after dose adjustments until control is achieved, then every 6–12 mo as indicated.
- Consider monitoring TSH level until normalized if it was elevated at initial diagnosis (refer to treatment and monitoring section above).
GROUP 2: DOGS WITH NO CLINICAL SIGNS OF HYPOTHYROIDISM AND A LOW TT4
Clinical Presentation
Group 2 dogs have no symptoms of hypothyroidism and a decreased TT4 on routine laboratory screening.
Next Steps
- It is critical to consider the dog’s signalment, such as age and breed, before proceeding with additional testing for hypothyroidism. Clinically normal dogs of certain breeds such as greyhounds, Alaskan sled dogs (particularly when racing), shar peis, salukis, and deerhounds are routinely reported to have TT4 concentrations that are lower than established laboratory reference ranges. The guidelines task force recommends using breed-specific reference ranges when interpreting hormone levels in these breeds, especially if no clinical signs are present.25
- Review current and previous medications. Drugs such as phenobarbital, clomipramine, toceranib phosphate, glucocorticoids, and sulfonamides are reported to lower TT4 and/or fT4 concentrations; TSH may be increased or within the reference range, depending on the mechanism of the effect on thyroid function. These changes are reversible in most cases once the medications are discontinued.18,26,27
- Investigate for nonthyroidal illness if the dog is sick. Euthyroid sick syndrome can decrease circulating thyroid hormone concentrations, with preferential impact on TT4. In severe illness, fT4 is also impacted. TSH may be subnormal or within the reference range.19 Ideally, further thyroid testing should be delayed until clinical illness has resolved and the dog is clinically well.
- Review symptoms of hypothyroidism with owner and consider measurement of fT4 and TSH levels if symptoms develop.
- Monitor for development of clinical signs.
GROUP 3: DOGS WITH CLINICAL SIGNS OF HYPOTHYROIDISM AND A NORMAL TT4
Clinical Presentation
Group 3 dogs have a similar clinical presentation to Group 1 dogs, but the TT4 does not confirm hypothyroidism.
Next Steps
- Investigate for other causes of clinical presentation by reviewing history with client and pursuing additional diagnostics.
- Perform an fT4ed with TSH and consider additional testing to rule out thyroiditis, specifically assessing for the presence of antithyroid autoantibodies. Dogs with thyroiditis can have antibodies that falsely elevate TT4 levels because of cross-reactivity of the T4 autoantibodies. Signs of hypothyroidism can develop slowly over time in some of these dogs.3
- A TSH response test could be considered if the TT4 or fT4 concentrations are in the low-normal reference range and the patient lacks circulating antithyroid antibodies.
- Dogs should be treated with supplementation if the diagnosis is confirmed, and therapy is monitored as described for Group 1. However, if the TT4 concentration was within reference range at diagnosis owing to the presence of T4 autoantibodies, an fT4ed is the preferred test to accurately monitor therapy.
The 2023 AAHA Selected Endocrinopathies of Dogs and Cats Guidelines are generously supported by Boehringer Ingelheim Animal Health, IDEXX, Merck, Zoetis, and Zomedica.



